Introduction
Cardiovascular disease (CVD) caused by atherosclerosis remains the leading cause of mortality worldwide, accounting for 30 percent of all global deaths (Reference Naghavi, Abajobir and Abbafati1). High low-density lipoprotein-cholesterol (LDL-C) leads to atherosclerosis and acts as the top prevention and treatment target for CVD (Reference Critchley, Liu, Zhao, Wei and Capewell2). In China, the disease burden of high LDL-C keeps increasing over the past 30 yr (Reference Du, Shi and Song3). Previous reports suggested that more than 70 percent of Chinese adults with high LDL-C are facing an extremely high risk of CVD (Reference Zhao, Wang and Mu4), but only 23 percent of all hospitalized patients with diabetes had their lipid profiles well controlled (Reference Hou, Yu and Li5).
Hydroxymethylglutaryl CoA (HMG-CoA) reductase inhibitors (statins) are the first-line treatment for primary and secondary prevention of CVD, and work by lowering the LDL-C levels (Reference Zhu, Gao and Zhao6;Reference Jellinger, Handelsman and Rosenblit7). Although the Western major guidelines recommended the second lipid-lowering drugs only after the maximally tolerated dose of statins (Reference Mach, Baigent and Catapano8–12), most clinicians and patients adopt low- to moderate-dose statins by concerning the potential side effects in China (Reference Liao13;Reference Tomlinson, Chan and Liu14). A recent global clinical practice guideline with its accompanied meta-analyses suggested that people with maximally tolerated statins at high risk of CVD may choose other lipid-lowering drugs including ezetimibe and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors based on the case-to-case benefit and harm balancing and values and preference of the patient (Reference Hao, Aertgeerts and Guyatt15–Reference Wang, Zhan and Du18).
Given the perspective of this recommendation is solely patient-centered, it does not consider the cost or the healthcare resource consumption, which is also infeasible from a global view. China has the largest population as well as those with established CVD (Reference Rehman, Rehman, Mumtaz and Jianglin19), but the per capita healthcare resource is limited and ranks 74 worldwide (Reference Bank20). Many reports suggested the price of PCSK9 inhibitors is beyond the willingness-to-pay (WTP) threshold in Western countries (Reference Kumar, Tonkin, Liew and Zomer21;Reference Ella, Danny and Andrew22). Both the Chinese healthcare system and the pharmacy industry are making every effort to reduce the annual cost of PCSK9 inhibitors. The National Healthcare Security Bureau reduced the price of PCSK9 inhibitors (Evolocumab and Alirocumab) by about 70 percent through the national bid-winning negotiation (23). However, it remains unclear whether the current price fits the Chinese healthcare system. This simulation study aimed to investigate the cost-effectiveness of adding ezetimibe and PCSK9 inhibitors to high-dose statins in China, based on the latest evidence synthesis.
Materials and methods
Populations
The model population is comprised of participants from a network meta-analysis (NMA) which contains 16 trials encompassing 111 098 patients (Reference Khan, Yedlapati and Lone16). This cost-effectiveness analysis study modeled people for the secondary prevention of CVD as the simulated population.
Therapeutic Regimens
Based on the Chinese context, this simulation study evaluated four therapeutic strategies including the high-dose statin-only group (atorvastatin 80 mg, once a day), ezetimibe plus statin group (atorvastatin 80 mg once a day, plus ezetimibe 10 mg once a day), PCSK9 inhibitors plus statin group (atorvastatin 80 mg once a day, plus PCSK9 inhibitors 420 mg once a month); PCSK9 inhibitors plus ezetimibe plus statin group (atorvastatin 80 mg once a day, plus ezetimibe 10 mg once a day, plus PCSK9 inhibitors 420 mg once a month).
Markov Model
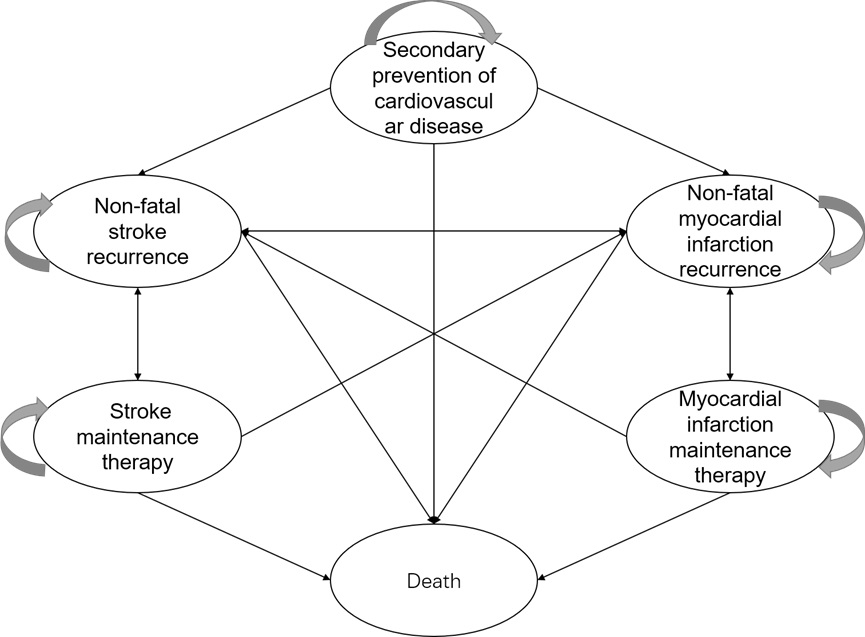
We constructed a Markov model, using TreeAge Pro 2022 (TreeAge Software, Williamstown, MA), from a healthcare system perspective. Six disease states of secondary prevention of CVD include recurrence of nonfatal stroke, recurrence of nonfatal myocardial infarction, maintenance therapy for myocardial infarction, maintenance therapy for stroke, and death (Supplementary Figure S1). Each patient runs for 20 cycles, to simulate the long-term cost-effectiveness for 20 yr after treatment with the half-cycle correction.
Model Assumptions
Due to data missingness, we were unable to obtain differences in event risks for CVD-related risks across different disease states, as well as differences in quality of life between patients in the secondary prevention of CVD. This long-term Markov model assumed: (i) the event risk ratio is fixed across different ages; (ii) the quality of life of patients in the secondary prevention of CVD stage is consistent with that of patients in the maintenance treatment of myocardial infarction (Reference Kumar, Tonkin, Liew and EJIJoC24).
Transition Probability
We adopted the probability estimates of transmission from a recent NMA (Reference Hao, Aertgeerts and Guyatt15), including the recurrence rate of nonfatal stroke, the recurrence rate of nonfatal myocardial infarction, cardiovascular mortality, and noncardiovascular related mortality in secondary prevention patients under each therapy (Supplementary Table S1) (Reference Li, Du and Wang17).
Cost
From the perspective of the healthcare system, this study considers the direct medical cost. The average drug consumption of the research groups is selected as the drug dosage. Due to data accessibility, the research chose the price of Evolocumab to be the price of PCSK9 inhibitors. The unit price was accessed from a central hospital in Sichuan Province which is available to the public. The price of statin used is the price of generic drugs (Reference Yao25–Reference Wang, Zhang, Jin, Liao and Dong28). To identify the relevant and timely parameters to form the model, we have comprehensively searched the major databases including PubMed, EMBase, and Scopus from inception to May 2022. Supplementary Table S3 showed the keywords for each item. The other costs were from literatures. The upper and lower limits of statin costs used are the cost of original drugs and 90 percent cost of generic drugs. The upper and lower limits of other drugs used ±10 percent of the base price. Previous publication informs the costs of cardiovascular events in the model after correcting with the consumer price index (CPI) (Reference Dryhurst, Schneider and Kerr31). We convert CNY to US$ with the average exchange rate in 2021, which was 6.45 (32). This study set the discount rate of both cost and utility at 5 percent with 0–8 percent as its lower and upper bounds in the sensitivity analysis (Reference Liu33). Table 1 illustrates the costs involved in this study and their sources, determination methods, and range.
Table 1. Base case and plausible ranges of model cost (USD)

Quality-of-Life and Utility Values
In this model, we estimate health output using health status-specific utility, measured by quality-adjusted life years (QALYs). Given the lack of data from China, a study from South Korea informs the study regarding the health status-specific utility data in people under the secondary prevention of CVD (Reference Kang, Park, Chae and Roh29). The utility value for each state in the first year after myocardial infarction and stroke recurrence were expressed by the utility values of the population when the disease was in the acute state, and the calculation formula was: recurrence state of the disease = maintenance therapy state of the disease × (1 − percentage of utility reduction). The reduction of the utility was from the previous study (Reference Yang, Li and Zhou30) (Table 1).
Threshold
In this study, three times the per capita GDP of China in 2021 is used as the WTP threshold. The National Bureau of Statistics shows the per capita GDP of China in 2021 was CNY 80,976 (US$12,551) (Reference Dryhurst, Schneider and Kerr31), and thus the threshold value set was CNY242,928 (US$37,655) per QALY gained.
Sensitivity Analyses
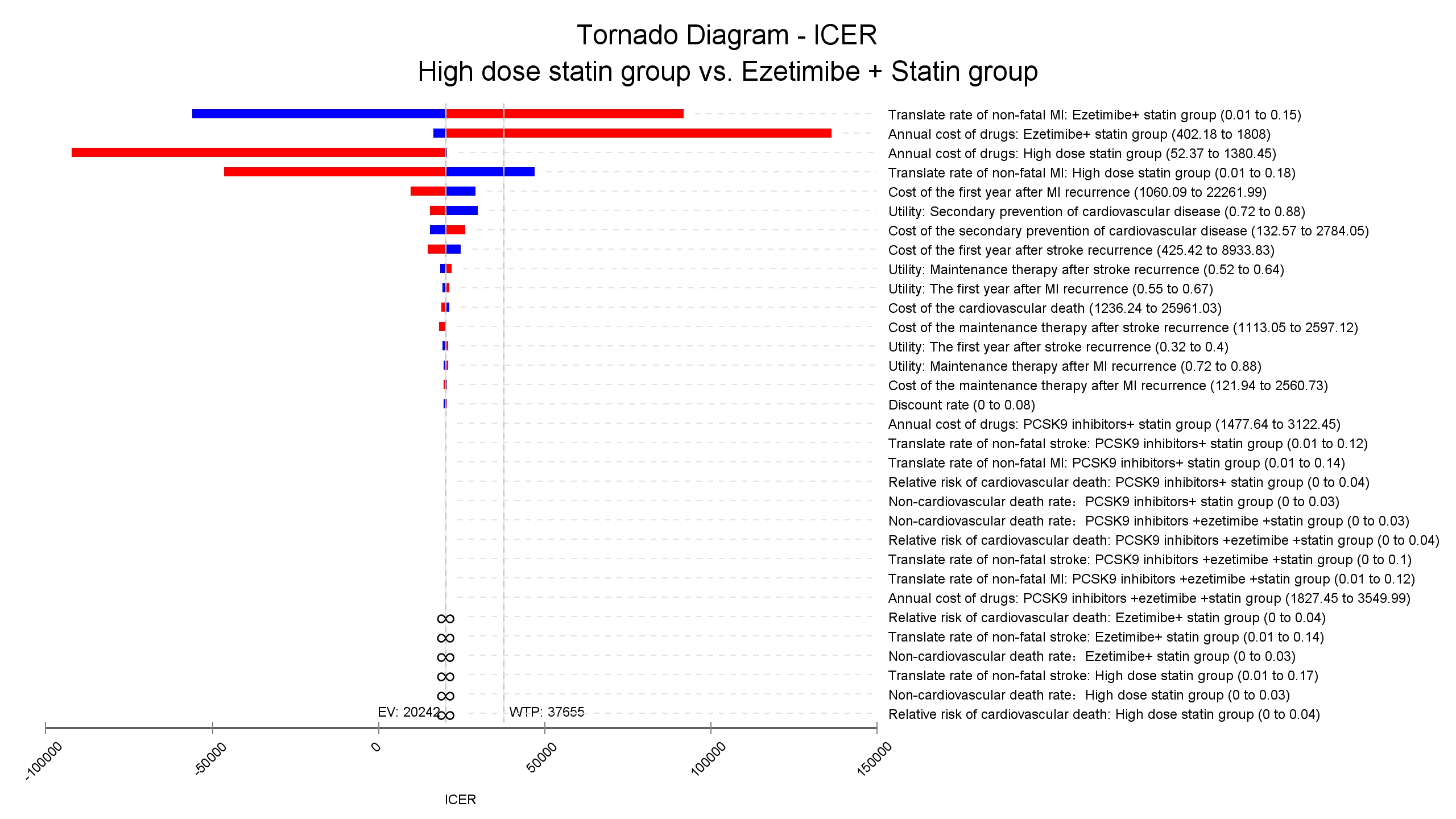
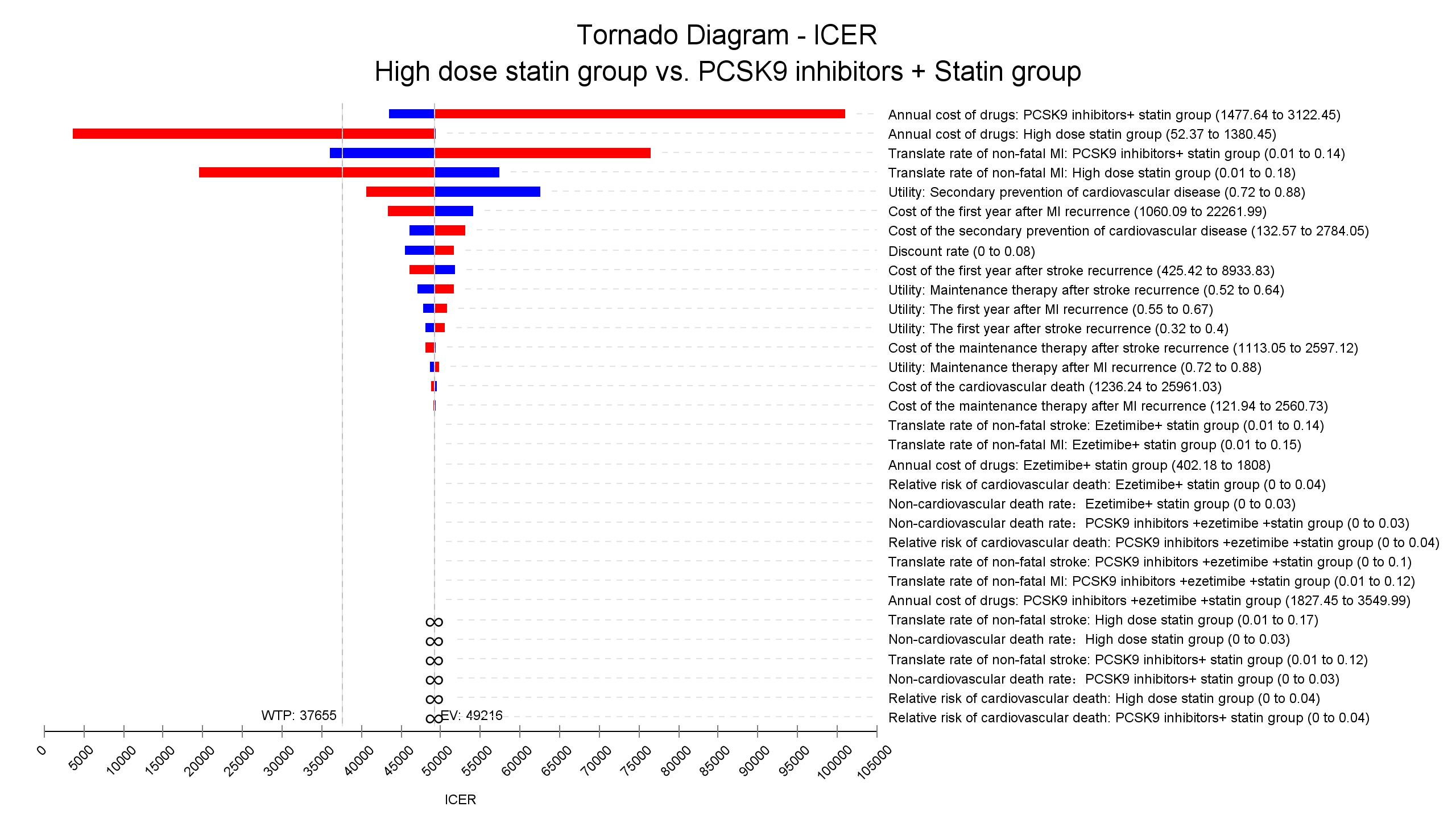
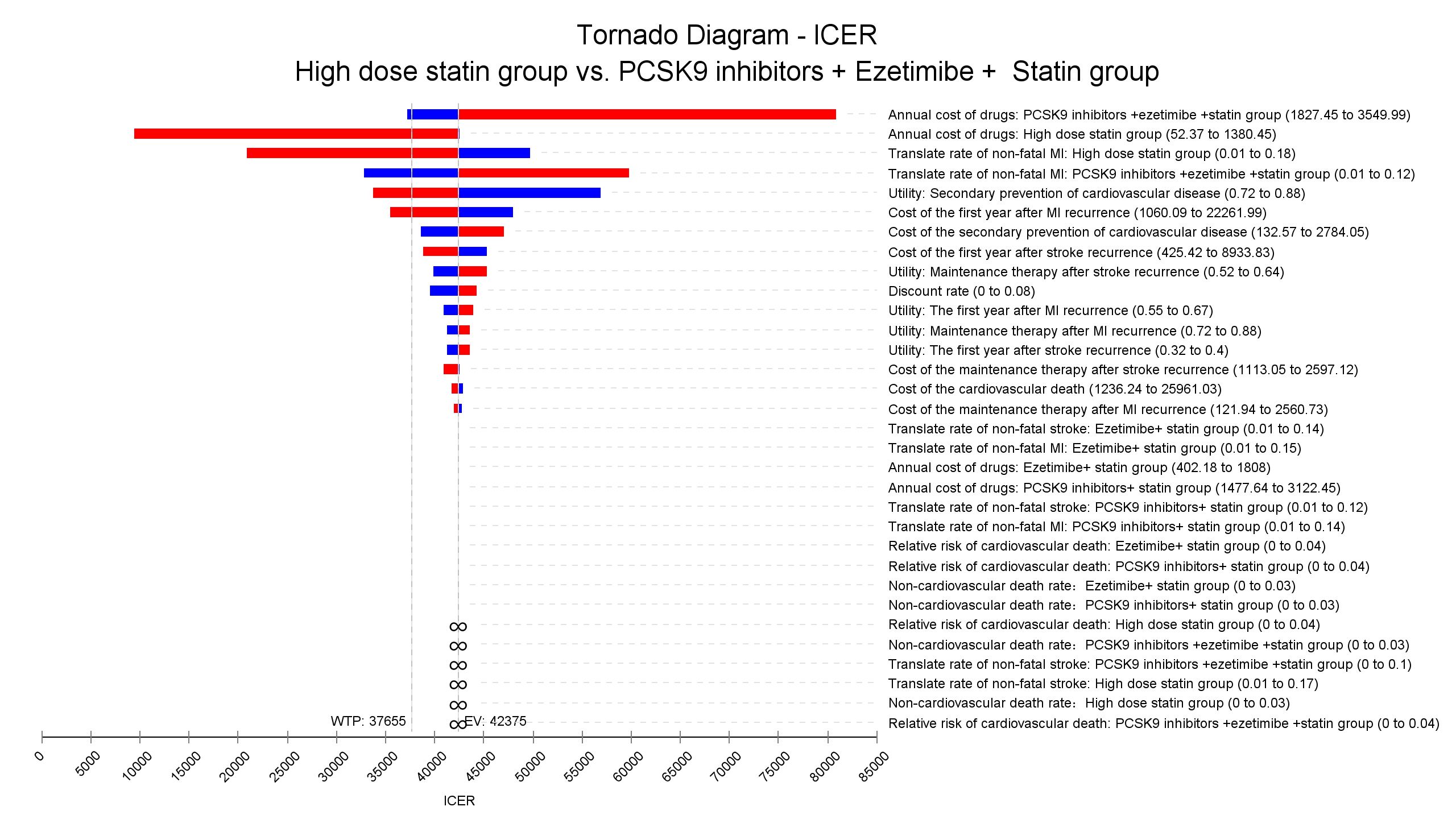
One-way sensitivity analyses are conducted in the models to test the robustness of the results considering the potential violation of the modeling assumptions or the variance of key model parameters. Depending on data availability, the ranges considered in the one-way sensitivity analyses include 95 percent confidence intervals or ± 10 percent of the base case values. The main indicators of one-way sensitivity analysis are the price of two drugs, the clinical outcome, the probability of each transfer, and the utility value of the two drugs after treatment. The results from the one-way sensitivity analyses are presented in a Tornado diagram (Supplementary Figures S2–S4), showing sequentially the variables with the largest impact on the cost-effectiveness results.
The overall impact of uncertainty in the model is assessed with probabilistic sensitivity analyses (PSA) by defining distributions for key parameters in the model. The key parameters included in the PSA are the clinical outcome, unit cost, and utility variables. An overall summary of the variables included in the PSA, and the distributions applied to these variables, is provided in Supplementary Table S2. We ran the PSA for 10,000 iterations for the simulation (Reference Hatswell, Bullement, Briggs, Paulden and Stevenson34), and the results are plotted on the cost-effectiveness plane (CEP) as scatterplots and cost-effectiveness acceptability curves (CEACs) to evaluate the pharmacoeconomic value of the four treatments.
Results
Base-case results for estimating the cost and effectiveness of statin, ezetimibe, and PCSK9 inhibitors are presented in Table 2 and Figure 1. PCSK9 inhibitors plus ezetimibe plus statin group had the highest cost, but also the highest utility gained compared to the other three groups. The ICER of ezetimibe plus statin versus high-dose statin is US$20,242 per QALY gained, which is below the WTP threshold. The ICER of PCSK9 inhibitors plus statin versus high-dose statin is US$68,910 per QALY gained, which is high above the WTP threshold. The ICER of PCSK9 inhibitors plus ezetimibe plus statin versus high-dose statin is US$51,552 per QALY gained, which is above the WTP threshold.
Table 2. Cost-effectiveness results for statin, ezetimibe, and PCSK9 inhibitors


Figure 1. Cost-effectiveness results for statin, ezetimibe, and PCSK9 inhibitors.
The one-way sensitivity analysis of the incremental cost-effectiveness ratio (ICER) is carried out within the range of all indicator changes (Supplementary Figures S2–S4). In all pairwise comparisons across two treatments, the transition rate of nonfatal MI of treatment and the annual cost of the treatment demonstrated the largest impact on the ICER. The probabilistic sensitivity analysis showed that the acceptability of ezetimibe plus statin was 53.1 percent, the acceptability of high-dose statin was 27.3 percent, the acceptability of PCSK9 inhibitors plus ezetimibe plus statin was 16.8 percent, and the acceptability of PCSK9 inhibitors plus statin was 2.9 percent under the current WTP threshold (Figure 2). Figure 3 shows the Monte Carlo simulation of the four strategies with 10,000 iterations.

Figure 2. Cost-effectiveness acceptability curve – High dose statin versus Ezetimibe + statin versus PCSK9 inhibitors + statin versus PCSK9 inhibitors + ezetimibe + statin.

Figure 3. Cost-effectiveness scatterplot of the four strategies: (A) Cost-effectiveness scatterplot – Ezetimibe + statin versus High dose statin, (B) Cost-effectiveness scatterplot – PCSK9 inhibitors + statin versus High dose statin, and (C) Cost-effectiveness scatterplot – PCSK9 inhibitors + Ezetimibe + statin versus High dose statin.
Discussion
Using the latest evidence synthesis and cost data, this simulation study compared the cost-effectiveness of four lipid-lowering regimens in Chinese adults under secondary prevention in the view of the healthcare system. High-dose statin plus ezetimibe showed the highest ICER in the corresponding population, while the cost of statins as well as the anticipated risk of myocardial infarction is impacting the results. A study conducted in the United States found that the ICER for PCSK9 inhibitors compared to statins for preventing cardiovascular events is US$268,637 per QALY (in 2017), which is cost-effective (Reference Fonarow, Keech and Pedersen35). A similar conclusion reached Canada with the ICER being US$48,912 per QALY (in 2021) by adding PCSK9 inhibitors (Reference Grégoire, Champsi and Jobin36). However, with an ICER of US$133,613 per QALY (in 2019), PCSK9 inhibitors in China were far from cost-effective when the decision threshold of three times of GDP (US$32,973 per QALY) (Reference Liang, Chen and Yang37). The difference could be attributable to the low GDP in China as well as the relative low cost for CVDs. Previous studies were based on the results of the FOURIER trial, which estimated the risk of various outcomes based on intervention strategies that lowered LDL-C values (Reference Hao, Aertgeerts and Guyatt15). However, the latest evidence suggests that LDL-C values do not have a linear relationship with clinical risk (Reference Johannesen, Langsted, Mortensen and Nordestgaard38;Reference Yuan, Huang and Ma39). Our finding is in line with previous reports but provides additional information with updated estimates (Reference Liang, Chen and Yang37).
The latest evidence demonstrates the effectiveness and safety of PCSK9 inhibitors and ezetimibe in the primary and secondary prevention of CVD (Reference Li, Du and Wang17;Reference Wang, Zhan and Du18). Nevertheless, the stakeholders in choosing lipid-lowering drugs are beyond clinicians and patients. In middle to low-income countries and those with restricted resources, the budget decides the healthcare equity at the population level. Although the bid-winning negotiation sharply cut the price of PCSK9 inhibitors in China, the add-on therapy with PCSK9 inhibitors on high-dose statins could be cost-effective only if there is a further 33.6 percent reduction in the annual cost of PCSK9 inhibitors (Evolocumab, from US$1,584 to US$1,052). Adding both ezetimibe and PCSK9 inhibitors to people receiving high-dose statins requests a 24.7 percent price reduction of the annual cost of PCSK9 inhibitors (Evolocumab, from US$1,584 to US$1,193) to meet cost-effective criteria. Nevertheless, different from the National Bureau criteria adopted in this study, the medical insurance negotiation policy in China set one-time GDP instead of 3-time GDP for the WTP cost anticipation. Under this circumstance, high-dose statins are the prioritized option in around 75 percent of cases, while the combination therapy with evolocumab may be acceptable in 20 percent of cases. The cost-effectiveness requests a 68.1 percent annual cost cut for PCSK9 inhibitors (US$506 per year) for adding PCSK9 inhibitors (Evolocumab) to high-dose statins and a 74.3 percent price cut (US$407 per year) for adding PCSK9 inhibitors (Evolocumab) and ezetimibe to high-dose statin.
The present study has some limitations. First, the base case is adopted from the trial population from an NMA rather than real-world Chinese people. It introduces the indirectness of the study population that previous reports suggested that the trial population may be heterogeneous with Chinese real-world people (Reference Zhou, Zhang and Zhang40). Nevertheless, the sensitivity analysis suggested that the population characteristics had a limited impact on the ICER and demonstrated the robustness of the results. Second, the study adopted utility data from Korea instead of China, making further indirectness. Nevertheless, China and Korea shared close cultures and ethnicity and the sensitivity did not identify the utility value to be the dominant factor for the ICER. Third, the current study did not consider the cost of the side effects, which is very different from other cost-effectiveness analyses. Nevertheless, high-quality systematic reviews demonstrated the safety of both drugs except for the injection-site reaction for PCSK9 inhibitors, which is not likely to cause additional costs (Reference Li, Du and Wang17;Reference Wang, Zhan and Du18). The study chose Markov model to simulate the disease development. Although the Markov model was widely used for cost-effectiveness analyses, the fixed transition probability limited the precision of the simulation and thus warrant cautious interpretation in real-world practice.
Conclusion
In conclusion, the regimen of ezetimibe plus statin is the most cost-effective in China. The results of this study will require updating with new evidence and changes in health policy in the future.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0266462323000296.
Author contribution
Y.X. performed the statistical analysis and drafted the manuscript. S.L. handled funding and drafted the manuscript. L.G. and H.D. acquired and interpreted the data. B.A. and Q.H. provided technology support and made critical revision to the manuscript. M.H. and S.L. conceived the overall study, acquired the data, and made critical revision to the manuscript. S.L. and M.H. contributed equally to this work and should be considered co-corresponding authors. All authors have reviewed and approved the manuscript and agree with submission to International Journal of Technology Assessment in Health Care.
Funding statement
This study was supported by the Chinese Cardiovascular Association-Access fund (Grant No. 2019-CCA-ACCESS-103). The funders are not involved in the analysis and interpretation of the data or in the decision to publish the results.
Competing interest
The authors declare none.