Case
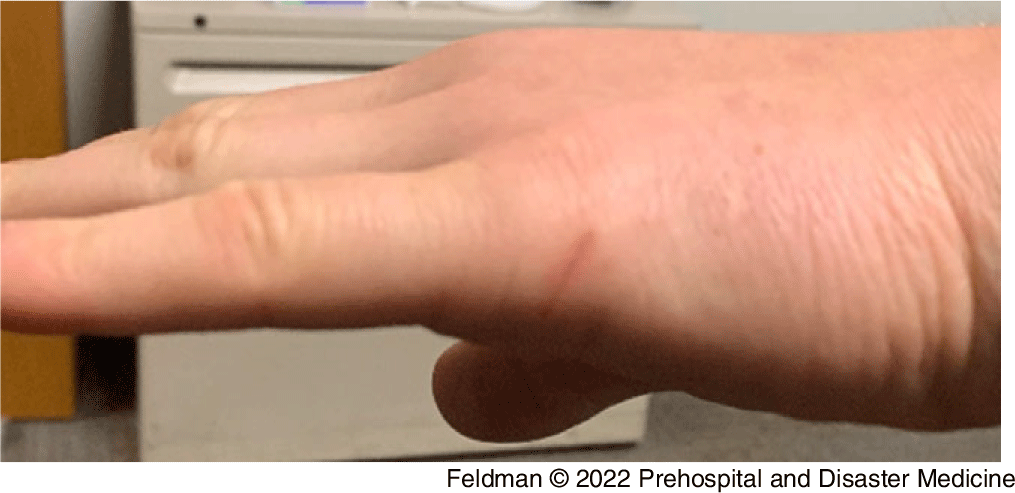
A 32-year-old opioid naïve male (author RF) weighing 89kg presented for evaluation 20 minutes after a dermal exposure to approximately 380mcg of fentanyl (38ml of 10mcg/ml fentanyl solution). The patient was working as an emergency medicine pharmacist and was attempting to dispose of a container with 950mcg of aqueous fentanyl (95ml x 10mcg/ml). When removing tubing from the container, liquid fentanyl was released onto the ungloved hand, wrist, and forearm of the patient (Figure 1). Some fentanyl then spilled from the arm onto the ground. It was determined afterward that the container had 570mcg remaining (57ml) suggesting a total potential exposure of 380mcg (38ml) to the hand and forearm. The exposed hand had a one-centimeter healing laceration 1.5cm proximal to the fifth digit on the dorsum of the affected hand (Figure 2) and a 0.5cm abrasion on the volar aspect of the affected wrist (Figure 1). The estimated exposure surface area was approximately 0.5%-2.0% of the total body surface area. Reference Rhodes and Phillips1

Figure 1. Hand and Wrist Visibly Soiled with Fentanyl.
Note: Larger liquid volumes appear more visible, however nearly full surface area was exposed. Arrow shows 0.5cm abrasion.

Figure 2. Location of One-Centimeter Healing Laceration During Exposure.
Approximately one minute after the exposure, the patient washed the exposed area with soap and water for 60 seconds. Occupational accident procedures were followed and a brief medical exam was performed. The patient remained alert and oriented and endorsed no mental status changes. Pupillary exam revealed 6mm pupils that were reactive to 4mm with light. Vital sign assessment demonstrated a heart rate of 61 beats per minute, a blood pressure of 129/92mmHg, respiratory rate of 12/minute, and an oxygen saturation of 100% on room air. The patient developed no immediate or subsequent symptoms of opioid exposure and resumed work without incident after initial evaluation. Informed consent from the patient was obtained to publish this report.
Discussion
The high prevalence of fentanyl in the illicit drug supply has generated concern among first responders regarding occupational exposure. Surveys of first responder perceptions report the majority believe death can occur from brief fentanyl dermal contact. Reference Del Pozo, Sightes, Kang, Goulka, Ray and Beletsky2–Reference Winograd, Phillips and Wood4 Stories of supposed fentanyl overdoses in first responders that are largely unconfirmed but widely distributed by social media may be contributing to an inaccurate risk perception regarding brief fentanyl exposure. Reference Beletsky, Seymour and Kang5 Symptoms in these media reports often develop instantly after exposure and are inconsistent with an opioid toxidrome. Reference Beletsky, Seymour and Kang5 Additionally, the actual substance involved in these reports may go unconfirmed. Many of the symptoms in these unsubstantiated overdoses are more consistent with a psychosomatic response than with fentanyl toxicity. Reference Beletsky, Seymour and Kang5
Properties of dermally absorbed drugs include adequate lipophilicity to penetrate outer skin layers (eg, stratum corneum) and small molecular size to facilitate rapid diffusion. Reference Larsen, Nielsen, Sørensen and Nielsen6 The high lipophilicity and low molecular weight of fentanyl does make it a candidate for dermal absorption. However, it is not absorbed instantaneously and thus symptoms do not occur instantaneously as sometimes reported in media. Lipophilic drugs must first penetrate the avascular stratum corneum, which fentanyl does rapidly. The compound then remains in this avascular lipophilic tissue as a depot while slower systemic absorption into vascularized aqueous tissue occurs, thus limiting systemic absorption. Reference Larsen, Nielsen, Sørensen and Nielsen6 In vitro studies demonstrate a lag time of 20 minutes for fentanyl to penetrate through skin and become present systemically. Reference Roy and Flynn7 Rapid dermal absorption does not appear possible without compromised skin barriers or specialized solvents. Prolonged contact is needed for continued absorption, and brief dermal exposures to aqueous fentanyl, powdered fentanyl, or its analogs is extremely unlikely to cause toxicity. Reference Larsen, Nielsen, Sørensen and Nielsen6 Moreover, use of gloves as recommended by the American College of Medical Toxicology (Phoenix, Arizona USA) and the American Academy of Clinical Toxicology (McLean, Virginia USA) joint statement on occupational fentanyl exposure further limits exposure risk. Reference Moss, Warrick and Nelson8
This case example is not representative of all dermal opioid exposures. The quantity of fentanyl that is present in illicit drugs may vary widely. Emergency medical personnel may encounter larger doses than reported in this case, or exposure to fentanyl in other pharmaceutical forms, such as a patch. The quantity of fentanyl absorbed is dependent on the dose exposed to and surface area available for absorption. In the case of a patch, fentanyl absorption is controlled by a matrix within the patch that limits the diffusion rate. Despite a very large reservoir of fentanyl within the patch (12,400mcg of fentanyl within a 100mcg/hour patch), it covers a small surface area (100mcg/hour patch covers 44cm2, approximately one-tenth of a 450cm2 hand) and fentanyl diffusion from the reservoir is controlled via the patch matrix. Reference Rhodes and Phillips1,9 Thus brief exposure to a patch is unlikely to cause acute toxicity, however the kinetics are not directly applicable to an exposure of aqueous or powdered fentanyl.
Brief dermal exposures to even larger amounts of liquid or aqueous fentanyl than reported in this case would still be unlikely to cause toxicity. To cite an extreme example for illustrative purposes, calculations from in vitro modeling with carfentanil (more lipophilic) at extremes of exposure (“infinite” dose model providing continued absorptive gradient, and using maximum observed flux rates) demonstrated the drug would need two minutes of exposure to the full palmar hand surface area of each hand to absorb a biologically relevant dose and up to 44 minutes to absorb a lethal dose. Reference Lent, Maistros and Oyler10 Thus, it appears even with a larger dose, larger surface area, and more potent opioid exposure, rapid decontamination should significantly mitigate risk.
Conclusion
Despite available evidence, the belief that even limited dermal fentanyl exposure may lead to death has a prevalence of 79%-80% among surveyed first responders. Reference Del Pozo, Sightes, Kang, Goulka, Ray and Beletsky2–Reference Winograd, Phillips and Wood4 A limitation in combatting misinformation about exposure is the lack of literature documenting outcomes from confirmed accidental fentanyl exposures. This case details a relatively large surface area dermal exposure to a large dose of analytically confirmed pharmaceutical fentanyl. Additionally, the exposure occurred at a site with some skin barrier compromise, a factor that reduces stratum corneum and can increase fentanyl absorption 30-fold at the site. Reference Roy and Flynn7 The patient underwent appropriate decontamination, had a brief medical assessment, and no clinical effects of opioid exposure were observed.
This information is of value to first responders and other health care workers who are at risk of occupational fentanyl exposure. In the event of an ungloved exposure, decontamination should be performed as soon as possible. In this case, no symptoms developed. Findings are consistent with in vitro and ex vivo data supporting low risk of rapid absorption after brief dermal fentanyl exposure.
Conflicts of interest/funding
The authors of this paper have no conflicts to disclose. There was no funding for this research.