



Introduction
Sleep disturbance is a universal experience during the pregnancy and postpartum periods (Lee, Reference Lee1998; Sivertsen, Hysing, Dørheim, & Eberhard-Gran, Reference Sivertsen, Hysing, Dørheim and Eberhard-Gran2015), and causes include: (1) sleep disruption and deprivation caused by physiological changes (e.g., hormonal changes, foetus growth, increased sleep disordered breathing and restless legs syndrome) and postpartum nighttime infant care (Bei, Coo, & Trinder, Reference Bei, Coo and Trinder2015), and (2) symptoms of insomnia (e.g., persistent difficulties in initiating and maintaining sleep), which about 60% individuals experience by the third trimester (Sivertsen et al., Reference Sivertsen, Hysing, Dørheim and Eberhard-Gran2015). In about half of the individuals with probable insomnia during pregnancy, symptoms of insomnia persist into at least 2 years postpartum (Sivertsen et al., Reference Sivertsen, Hysing, Dørheim and Eberhard-Gran2015).
Sleep disturbance is linked to a range of negative consequences. In community samples, sleep disturbance in the perinatal periods is associated with symptoms of depression and anxiety (Bei et al., Reference Bei, Coo and Trinder2015; Bei, Milgrom, Ericksen, & Trinder, Reference Bei, Milgrom, Ericksen and Trinder2010), impaired daytime functioning (McBean & Montgomery-Downs, Reference McBean and Montgomery-Downs2013; Wilson et al., Reference Wilson, Wynter, Anderson, Rajaratnam, Fisher and Bei2019), gestational diabetes (Facco et al., Reference Facco, Grobman, Reid, Parker, Hunter, Silver and Zee2017), pre-term births (Felder, Baer, Rand, Jelliffe-Pawlowski, & Prather, Reference Felder, Baer, Rand, Jelliffe-Pawlowski and Prather2017), as well as prolonged labour and higher rates of caesarean delivery (Lee & Gay, Reference Lee and Gay2004). In individuals who had insomnia disorder during pregnancy, poorer sleep during the postpartum was associated with lower sensitivity towards the infant (King, Rangel, Simpson, Tikotzky, & Manber, Reference King, Rangel, Simpson, Tikotzky and Manber2019); in individuals vulnerable for bipolar disorder, sleep loss is linked to risk of postpartum psychosis (Sharma & Mazmanian, Reference Sharma and Mazmanian2003).
Cognitive behavioural therapy for insomnia (CBT-I) is an effective treatment, with comparable short-term and superior long-term effects to sleep medication alone (Morin et al., Reference Morin, Vallières, Guay, Ivers, Savard, Mérette and Baillargeon2009). When factors outside one's control interfere with sleep (e.g., chronic pain, cancer), CBT-I still reduces insomnia severity (Smith, Huang, & Manber, Reference Smith, Huang and Manber2005). This is because CBT-I targets and alters behaviours and cognitions that play key roles in the maintenance of poor sleep, regardless of initial triggers. For example, going to bed early when not sleepy is a common unhelpful behaviour stemming from an effort to ‘make up’ for sleep loss, and this could strengthen the association between bed and wakefulness (in place of sleep); catastrophizing after a night of poor sleep could increase anxiety about sleep and negatively affect subsequent sleep. Cognitive behavioural strategies are highly relevant to the perinatal periods, because the significant sleep disruptions caused by physiological changes and infant care leave new parents particularly vulnerable to developing these unhelpful behaviours and cognitions.
A few recent randomised controlled trials (RCTs) tested the feasibility and efficacy of cognitive behavioural sleep interventions in the perinatal periods. All trials showed good acceptability and feasibility, but efficacy varied depending on whether the sample had existing insomnia complaints and intervention content and intensity.
In 179 individuals diagnosed with insomnia disorder during pregnancy, we showed that five sessions of in-person CBT-I were efficacious in reducing insomnia (Manber et al., Reference Manber, Bei, Simpson, Asarnow, Rangel, Sit and Lyell2019). Two other RCTs in individuals with prenatal insomnia symptoms or disorders showed that digitally delivered CBT-I also reduced insomnia (Felder, Epel, Neuhaus, Krystal, & Prather, Reference Felder, Epel, Neuhaus, Krystal and Prather2020; Kalmbach et al., Reference Kalmbach, Cheng, O'Brien, Swanson, Sangha, Sen and Drake2020). These trials indicate that CBT-I is effective for insomnia during pregnancy.
However, mixed findings were reported by studies of community samples that do not selectively target individuals with elevated insomnia symptoms and used mainly psychoeducational intervention with selective components of CBT-I. A pilot RCT in 40 first-time mothers delivered behavioural-educational sleep intervention via an in-person group during pregnancy, postpartum phone calls and written materials; the study found that intervention was well accepted, but differences in maternal sleep between intervention and control conditions were small or non-significant at 6 and 12 weeks postpartum (Sweeney, Signal, & Babbage, Reference Sweeney, Signal and Babbage2020). A larger RCT in 215 healthy first-time mothers delivered an intervention via two in-person group sessions during pregnancy along with written materials; the study found no effect of the intervention on maternal sleep at 6 weeks or 10 months postpartum, although the intervention group had greater improvement in sleep quality and insomnia symptoms at 4 months postpartum (small effect; Kempler, Sharpe, Marshall, & Bartlett, Reference Kempler, Sharpe, Marshall and Bartlett2020).
Current study
The existing literature shows that CBT-I is an effective treatment for clinically significant insomnia during pregnancy, but there are limited data to support it being delivered to all expectant individuals. Population-based studies showed that sleep problems are highly prevalent and distressing in this population (Dørheim, Bondevik, Eberhard-Gran, & Bjorvatn, Reference Dørheim, Bondevik, Eberhard-Gran and Bjorvatn2009; Sivertsen et al., Reference Sivertsen, Hysing, Dørheim and Eberhard-Gran2015). Even subclinical insomnia symptoms during the perinatal periods may warrant attention, as they were shown to persist over time, and sometimes worsen to clinical levels (Sedov & Tomfohr-Madsen, Reference Sedov and Tomfohr-Madsen2021).
Further, most trials either focused primarily on pregnancy outcomes (Felder et al., Reference Felder, Epel, Neuhaus, Krystal and Prather2020; Manber et al., Reference Manber, Bei, Simpson, Asarnow, Rangel, Sit and Lyell2019), or had short (up to 3 months; Kalmbach et al., Reference Kalmbach, Cheng, O'Brien, Swanson, Sangha, Sen and Drake2020; Sweeney et al., Reference Sweeney, Signal and Babbage2020) or medium (10 months; Kempler et al., Reference Kempler, Sharpe, Marshall and Bartlett2020) postpartum follow-up. No study to date has examined the long-term effects of CBT-I-based intervention on outcomes at or past the first postpartum year.
Also, given the high prevalence of sleep complaints during the perinatal periods, there is a critical need for an intervention that balances effectiveness and scalability, and can be integrated into routine perinatal care. Traditional multi-session face-to-face CBT-I is inefficient to reach the broader community. Meta-analysis showed that although self-help CBT-I is effective in reducing insomnia symptoms, supplementing self-help materials with therapist support enhances outcomes (Ho et al., Reference Ho, Chung, Yeung, Ng, Kwan, Yung and Cheng2015). Further, brief, single-session CBT-I with self-help pamphlets has been shown to be effective in reducing insomnia (Ellis, Cushing, & Germain, Reference Ellis, Cushing and Germain2015).
Therefore, the current trial adapted a cognitive behavioural sleep intervention for use in a community sample of expectant individuals. To increase scalability, the intervention was delivered via a front-loaded single session with a therapist, followed by self-help materials delivered at individualised perinatal milestones with ongoing email/phone support if needed. We evaluated the efficacy of the intervention relative to an attention- and time-matched control condition in an RCT, with longitudinal assessments conducted at seven different time points, from the third trimester of pregnancy to 2 years postpartum. The pregnancy endpoint was the first post-baseline assessment in late third trimester, and the postpartum endpoint was the first post-intervention assessment at 6 months postpartum. Group differences at other time points were exploratory. It was hypothesised that:
1. It would be feasible to integrate such an intervention in routine perinatal care, and the intervention will be acceptable.
2. Compared to the control group, the intervention group would report significantly better sleep quality (primary outcome), and secondarily, significantly better sleep-related functioning and lower symptoms of depression and anxiety at both the pregnancy and postpartum endpoints. Symptoms of depression and anxiety were included as secondary outcomes because they were well documented to share bi-directional associations with sleep disturbance (Alvaro, Roberts, & Harris, Reference Alvaro, Roberts and Harris2013).
Methods
Study design
The SEED (Sleep Eat Emotions and Development) project was a two-arm, parallel-group, single-blind, superiority RCT, carried out at a centrally located public hospital in Victoria, Australia. Ethical approvals were obtained from the Royal Women's Hospital and Monash University Human Research Ethics Committee. Methodologies are summarised below, with full protocol published elsewhere (Bei et al., Reference Bei, Pinnington, Shen, Blumfield, Drummond, Newman and Manber2019), and trial registered with the Australian New Zealand Clinical Trial Registry (ACTRN12616001462471).
Participants
Participants were expectant individuals enrolled in Childbirth Education. Inclusion criteria were: (a) nulliparas to test efficacy without confounds such as having older child(ren); (b) aged 18 or above; (c) singleton pregnancy; (d) English literacy; (e) regular access to email and Internet.
Exclusion criteria were: (a) current use of sleep-altering medications or substance; (b) current medical conditions (e.g., severe migraine) that directly affect sleep; (c) significant symptoms of sleep apnoea, periodic limb movement disorder, restless legs syndrome or circadian rhythm sleep-wake disorders; these physiologically-based sleep disorders were confounders not addressed in the intervention; insomnia disorder was not excluded; see protocol (Bei et al., Reference Bei, Pinnington, Shen, Blumfield, Drummond, Newman and Manber2019) for details; (d) work night shift; (e) mental health conditions: major depressive disorder (current); posttraumatic stress disorder (current); panic disorder if associated with nocturnal panic attacks >4 times in the past month; bipolar disorder (lifetime); psychotic disorders (lifetime); substance use disorders (during pregnancy).
All participants gave informed consent.
Randomisation and masking
Eligible participants were randomised 1:1 to the intervention (CBT) or a comparison condition (CTRL) using block randomisation with random block sizes of 4, 6 and 8 generated using an online tool (www.randomization.com). Participant allocation was stored in a database and only accessed by the research assistant (RA) who conducts the interview after eligibility was established; this RA was not involved in the rest of the trial. Other RAs who conducted post-baseline diagnostic interviews were blinded to treatment conditions; at the start of each interview, participants were asked to refrain from revealing which intervention materials they received. Participants, staff involved in intervention delivery and the data analyst were not blinded to treatment condition.
Procedures
All individuals enrolled in singleton pregnancy Childbirth Education classes were invited via a one-off email to ‘a research study that aims to evaluate the benefits of two well-being programs for new mothers’. Participants who provided informed consent were telephone screened using the M.I.N.I. International Neuropsychiatric Interview 7.0 (Sheehan et al., Reference Sheehan, Lecrubier, Harnett Sheehan, Janavs, Weiller, Keskiner and Dunbar1997) for DSM-5 psychiatric disorders (American Psychiatric Association, 2013) to rule out severe psychiatric conditions, and the Duke Structured Interview for Sleep Disorders (DSISD; Edinger et al., Reference Edinger, Wyatt, Olsen, Stechuchak, Carney, Chiang and Radtke2009) to rule out sleep disorders. Eligible participants were randomised.
Interventions were delivered across six time points (T1–T6), and outcomes were measured across seven time points (T1–T8 but not T3; see Table 1). Therapist-assisted component was delivered via telephone at T1, and as required via email or telephone between T1 and T6. Written intervention materials were delivered via email based on gestational milestones. Assessments were conducted via telephone and online surveys. Telephone interviews and interventions were recorded for reliability and treatment fidelity. After completing treatment (T6), participants were invited to re-consent for 1- and 2-year follow-up assessments (T7 and T8). Participants received vouchers at AUD$50, $100, $50 and $20 at T3, T6, T7 and T8, respectively.
Table 1. Timing of assessments and intervention

Note. Assessment at T1 is conducted immediately before intervention commenced. Assessments at T2, T4–T6 are conducted 1 week after the delivery of intervention materials. w, weeks; m, months.
All participants receive treatment as usual.
CBT sleep intervention
Key components included: (a) general skills for resilience towards sleep challenges: sleep hygiene, identifying and addressing unhelpful thoughts and beliefs about sleep, relaxation, calming the mind at bedtime; (b) understanding the difference between symptoms of insomnia and sleep deprivation; managing sleep initiation and maintenance difficulty using stimulus control (Manber et al., Reference Manber, Bei, Simpson, Asarnow, Rangel, Sit and Lyell2019); time-in-bed restriction was not included due to the community (rather than insomnia) sample; (c) typical sleep patterns of new parents and infants; realistic expectations and normalising some sleep loss; (d) mindfulness-based strategies targeting physical discomfort, pain and cognitive arousal; (e) strategies to promote infant self-soothing to reduce infant awakenings and increase maternal sleep efficiency; (f) prioritising own sleep, rest and self-care, enlisting partner and family support; (g) appropriately timed naps based on sleep and circadian rhythm principles; (h) managing sleepiness/fatigue.
Content was delivered via the following combined: (1) A 50 min, standardised telephone session was delivered by two registered psychologists at the start of the intervention. The psychologists were trained by BB, with regular peer consultations; audio recordings of sessions were reviewed weekly by BB to ensure treatment fidelity. The psychologist introduced the rationale underlying recommendations, personalised strategies based on each individual's needs, and encouraged consistent application of strategies to promote sustainable behavioural change. (2) A series of visually appealing emails containing text, graphics or audio-based intervention components were delivered at T1–T6, targeting sleep challenges specific to each time point (e.g. managing insomnia, physical discomfort and expectation of postpartum sleep at T1 and T2, managing daytime sleepiness at T3–T5, infant sleep and settling at T2–T6). (3) Participants who had difficulty applying the strategies could request brief email or telephone clarification from the psychologist.
Control intervention
To control for non-specific effects of participation in a well-being program, we chose ‘Healthy Diet’ as a control. It has the face validity of promoting ‘perinatal well-being’, and was delivered using the same method (i.e., same timing, frequency, quantity of written information and staff contact). Although diet may indirectly affect sleep, previously reported effects of diet interventions on sleep were small and often inconclusive (Peuhkuri, Sihvola, & Korpela, Reference Peuhkuri, Sihvola and Korpela2012). The project was promoted as ‘Sleep, Eat, Emotions, and Development (SEED)’, to further promote the face validity of a ‘well-being’ project.
Content of the Healthy Diet intervention included: (a) nutrients during late pregnancy; (b) nutrition for breastfeeding; (c) weight management during the postpartum period; (d) introducing solid food for the infant; (e) family eating. A registered dietitian conducted a 50 min manualised telephone session at the start of the intervention. Participants who had questions could request brief email or telephone clarification from the dietitian. Intervention materials were delivered via automated emails at the same time points as in the sleep intervention (Table 1).
Outcomes
Feasibility was assessed using recruitment/dropout rates and email opening rates. Acceptability was assessed using the Client Satisfaction Questionnaire (scores transformed to range 20–100, higher scores greater satisfaction; Attkisson & Zwick, Reference Attkisson and Zwick1982).
There were two primary outcomes, capturing two aspects of perinatal sleep quality: insomnia symptom severity was assessed using the Insomnia Severity Index (Bastien, Vallières, & Morin, Reference Bastien, Vallières and Morin2001) and sleep disturbance was assessed using the PROMIS Sleep Disturbance (Yu et al., Reference Yu, Buysse, Germain, Moul, Stover, Dodds and Pilkonis2011). Secondary outcomes include: DSM-5 Insomnia Disorder (without duration criteria) status from the DSISD (Edinger et al., Reference Edinger, Wyatt, Olsen, Stechuchak, Carney, Chiang and Radtke2009), self-report sleep patterns over the past week [total sleep time (TST) and sleep efficiency (SE)] from a modified Consensus Sleep Diary (Carney et al., Reference Carney, Buysse, Ancoli-Israel, Edinger, Krystal, Lichstein and Morin2012), sleep-related impairment (e.g., sleepiness, fatigue; Yu et al., Reference Yu, Buysse, Germain, Moul, Stover, Dodds and Pilkonis2011), and depression and anxiety symptoms (Pilkonis et al., Reference Pilkonis, Choi, Reise, Stover, Riley and Cella2011), with the latter three measured by PROMIS short forms. All measures were self-report instruments with strong psychometric properties. We chose measures well validated and normed for the general population, so that findings from this study in perinatal periods could be compared with adults in other life stages. For example, PROMIS scales form T scores, with a population mean of 50 and standard deviation of 10.
Adverse events were monitored during each assessment time point during the telephone interview. Participants were asked to report adverse effects immediately, and in addition, asked open-ended questions at T6 (end of intervention).
Primary and secondary outcomes were measured seven times (T1–T8 except T3; see Table 1). There were two primary endpoints: T2 as the pregnancy endpoint, and T6 (immediately post-intervention) as the postpartum endpoint.
Other measures
Participants' perceived credibility and expectancy of the intervention was measured using the Credibility Expectancy Questionnaire (Devilly & Borkovec, Reference Devilly and Borkovec2000) before commencing intervention, based on the description of intervention. The Dysfunctional Beliefs and Attitudes about Sleep Scale (DBAS; Morin, Vallières, & Ivers, Reference Morin, Vallières and Ivers2007) was administered at each time point, except T3. To promote face validity of the control condition, all participants were administered the Australian Eating Survey Food Frequency Questionnaire (Collins et al., Reference Collins, Burrows, Rollo, Boggess, Watson, Guest and Hutchesson2015) at T1 and T6 (data not reported here).
Statistical analysis
A priori power analyses based on t tests showed that 75 participants in each group provide >85% power (two-tailed α = 0.05) to detect a moderate effect (Cohen's d = 0.5).
Data were analysed in R 4.0.2 (R Core Team, 2020). All analyses were intention-to-treat and followed a pre-specified plan (Bei et al., Reference Bei, Pinnington, Shen, Blumfield, Drummond, Newman and Manber2019). Descriptive statistics were frequencies and percentages for categorical variables and means and standard deviations for continuous variables. Baseline group differences were tested using t tests or χ2 tests to document the success of randomisation.
Descriptive statistics described the feasibility and acceptability of the intervention (aim 1). To examine group differences in primary and secondary outcomes at each post-baseline time point (aim 2), separate multiple regression analyses were conducted with treatment condition as the independent variable, and the outcome as the dependent variable, adjusting for baseline levels of the outcome (Nunes et al., Reference Nunes, Pavlicova, Hu, Campbell, Miele, Hien and Klein2011). Effect sizes between conditions at each time point were adjusted, standardised mean differences, standardised by residual variance, comparable to within-person effects. Missing data were addressed using multiple imputation through chained equations in regression analyses (Little & Rubin, Reference Little and Rubin2002; van Buuren & Groothuis-Oudshoorn, Reference van Buuren and Groothuis-Oudshoorn2011). See online Supplementary for details.
Exploratory analyses repeated all primary analyses in participants who scored >7 on the ISI at baseline to explore intervention effects on those experiencing at least sub-clinical levels of insomnia symptoms at baseline.
Results
Between 5 May and 25 December 2016, 174 participants (100% female) gave informed consent, and were screened for eligibility (see participant flow in Fig. 1). A total of 163 completed the baseline assessments and were randomised to CBT (n = 81) or CTRL (n = 82). Among these, five (three in CBT, two in CTRL) dropped out before intervention commenced. Rates of missing data were low: among the 158 participants who started intervention, 65.8% completed all seven assessments, and 95.6% completed five or more assessments. Analyses below include all 163 randomised participants.
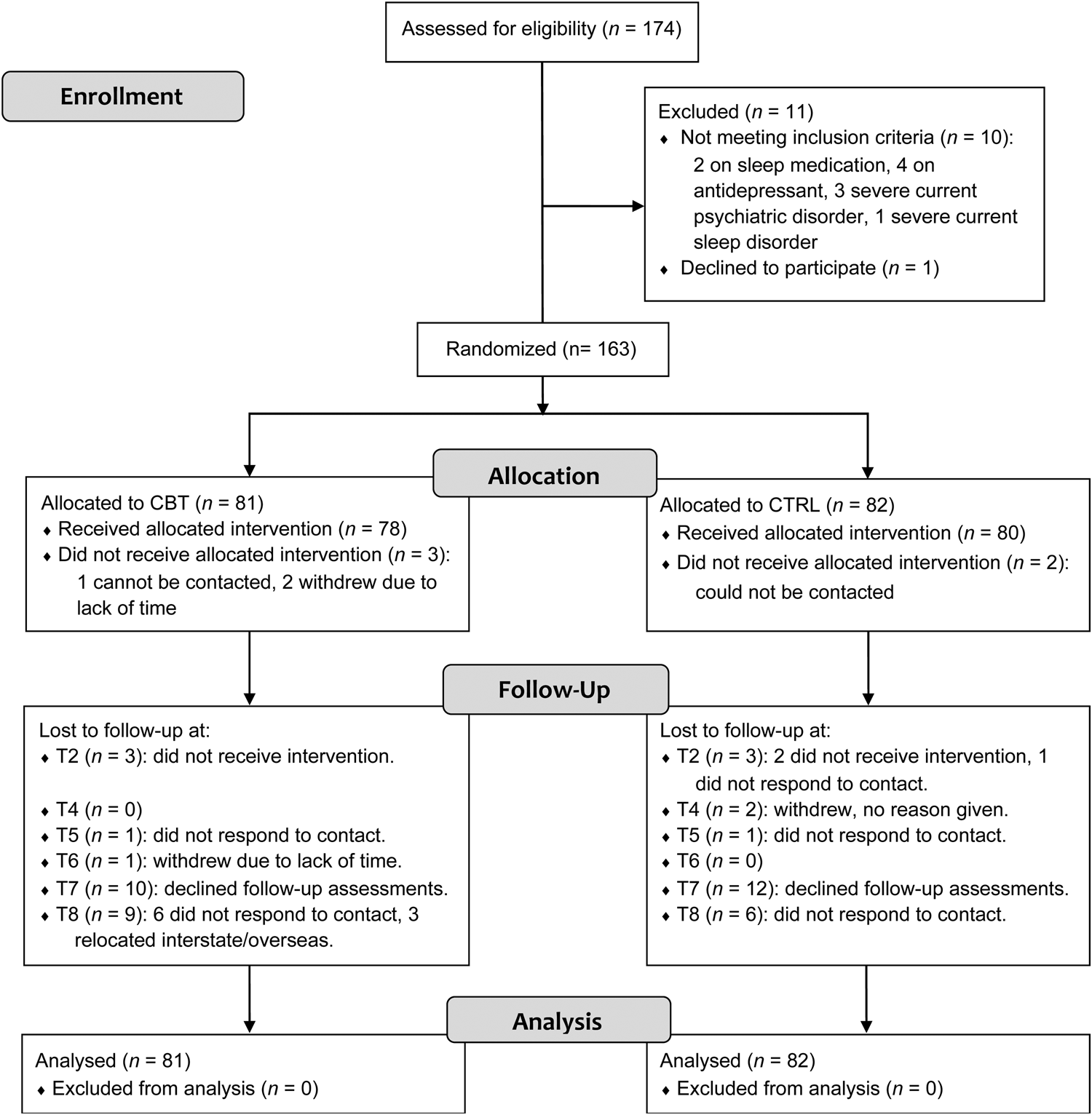
Fig. 1. Consort diagram of participant flow.
Note. CBT, cognitive behavioural therapy condition; CTRL, active control condition. T2 = 35 weeks' gestation, T3 (2 weeks postpartum) with no assessment is not shown, T4 = 6 weeks postpartum, T5–T8 = 3, 6, 12, 24 months postpartum, respectively.
Table 2 shows sample characteristics at baseline. Participants were aged 33.35 years (s.d. = 3.42) on average, 87.1% were Caucasian, most were married or in a de facto relationship (96.3%), working fulltime (77.3%) and had university education (89%). Most (73.6%) participants did not meet diagnostic criteria for any past or current mental health condition; 40 reported past (not current) history of a mental health condition (67.5% of these depression). The two intervention conditions did not differ significantly on any baseline characteristic (all p values ⩾ 0.12). Further, CBT and CTRL conditions had comparable scores on treatment credibility (p = 0.94), treatment expectancy (p = 0.73) and all baseline primary and secondary outcome measures (Table 2).
Table 2. Descriptive statistics of baseline sample characteristics
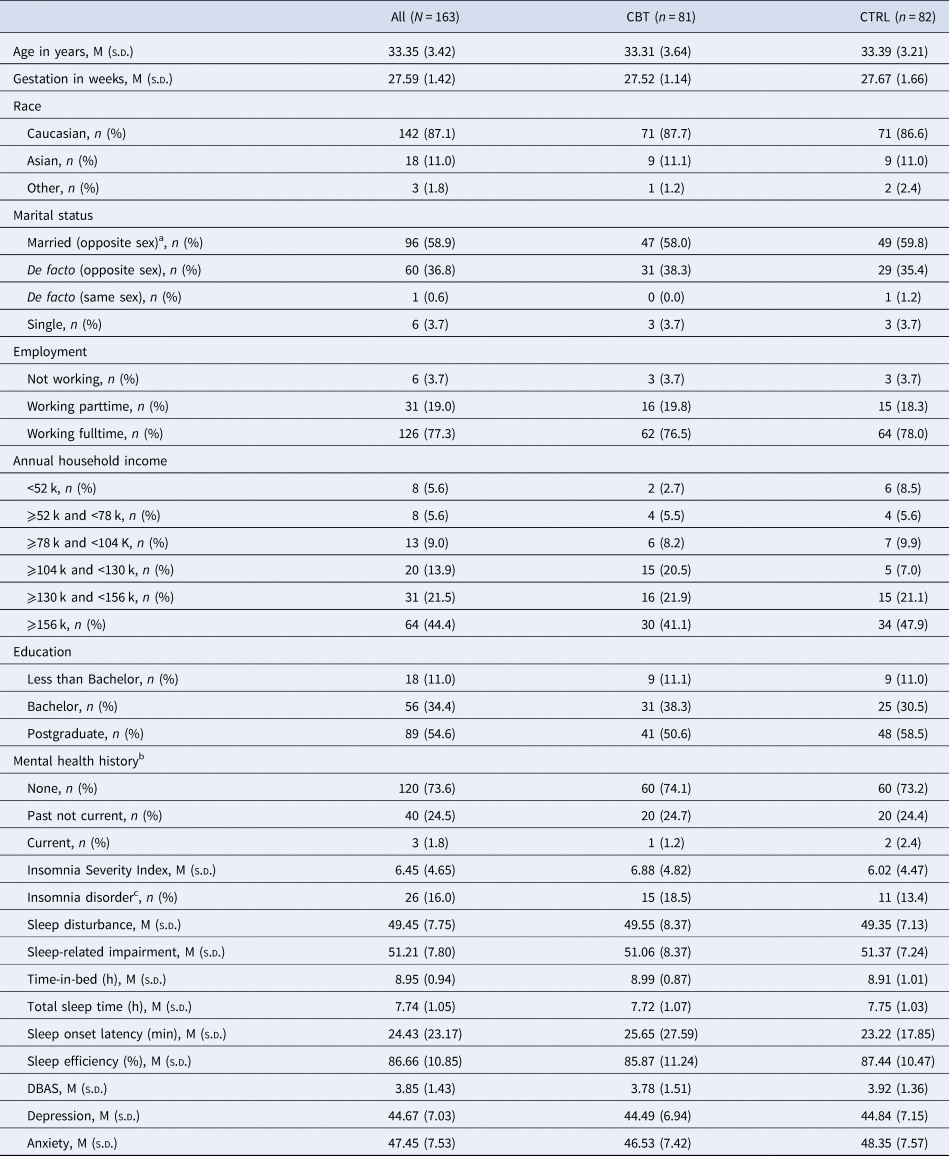
Note. M (mean) and s.d. (standard deviation) are presented for continuous variables, and n (%) are presented for categorical variables.
a All married participants were opposite sex as demographic information was collected in 2016, before same-sex marriage was legalised in Australia in 2017.
b Established using structured clinical interview.
c Meeting DSM-5 criteria for insomnia disorder without the duration criteria, assessed using structured clinical interview. DBAS, Dysfunctional Beliefs and Attitudes about Sleep. CBT (cognitive behavioural therapy) and CTRL (control) groups did not differ significantly on any of the above (p values range 0.12–0.99).
Feasibility and acceptability
A total of 1751 one-off email invitations were sent, 792 (45.2%) were opened, 304 (17.4%) were clicked on and 174 (9.9%) participants consented. Of the 163 participants randomised, 158 (96.9%) completed the telephone session. Intervention email opening rates were high for both the CBT (M = 82.3%, range: 77.8–88.1%) and CTRL (M = 87.1%, range: 77.4–95.7%) conditions. Of the 78 participants who started CBT, three (3.8%) requested further assistance to apply intervention strategies; each participant received one additional call of up to 50 min between T4 and T6. Two participants in CTRL requested additional information via one email correspondence. No adverse effects were reported in either condition. Satisfaction with both interventions was high, although participants were more satisfied with CBT (M ± s.d. = 81.17 ± 12.62) compared to CTRL (74.14 ± 14.01), p = 0.001. More participants in the CBT condition reported being ‘very’ or ‘mostly’ satisfied with the intervention compared to the CTRL condition (94.7% v. 81.6%, p = 0.013).
Primary outcomes
At the pregnancy endpoint (T2), participants in the CBT condition had significantly lower scores on the primary outcomes ISI [p = 0.001, effect size (ES) = 0.55] and PROMIS Sleep Disturbance (p < 0.001, ES = 0.56). At the postpartum endpoint (T6), the CBT condition had a lower average ISI compared to CTRL with a small effect size, but the difference was not statistically significant (p = 0.08, ES = 0.29); the two conditions did not differ significantly on PROMIS Sleep Disturbance (p = 0.52). Details are in Fig. 2 and online Supplementary Table S1.
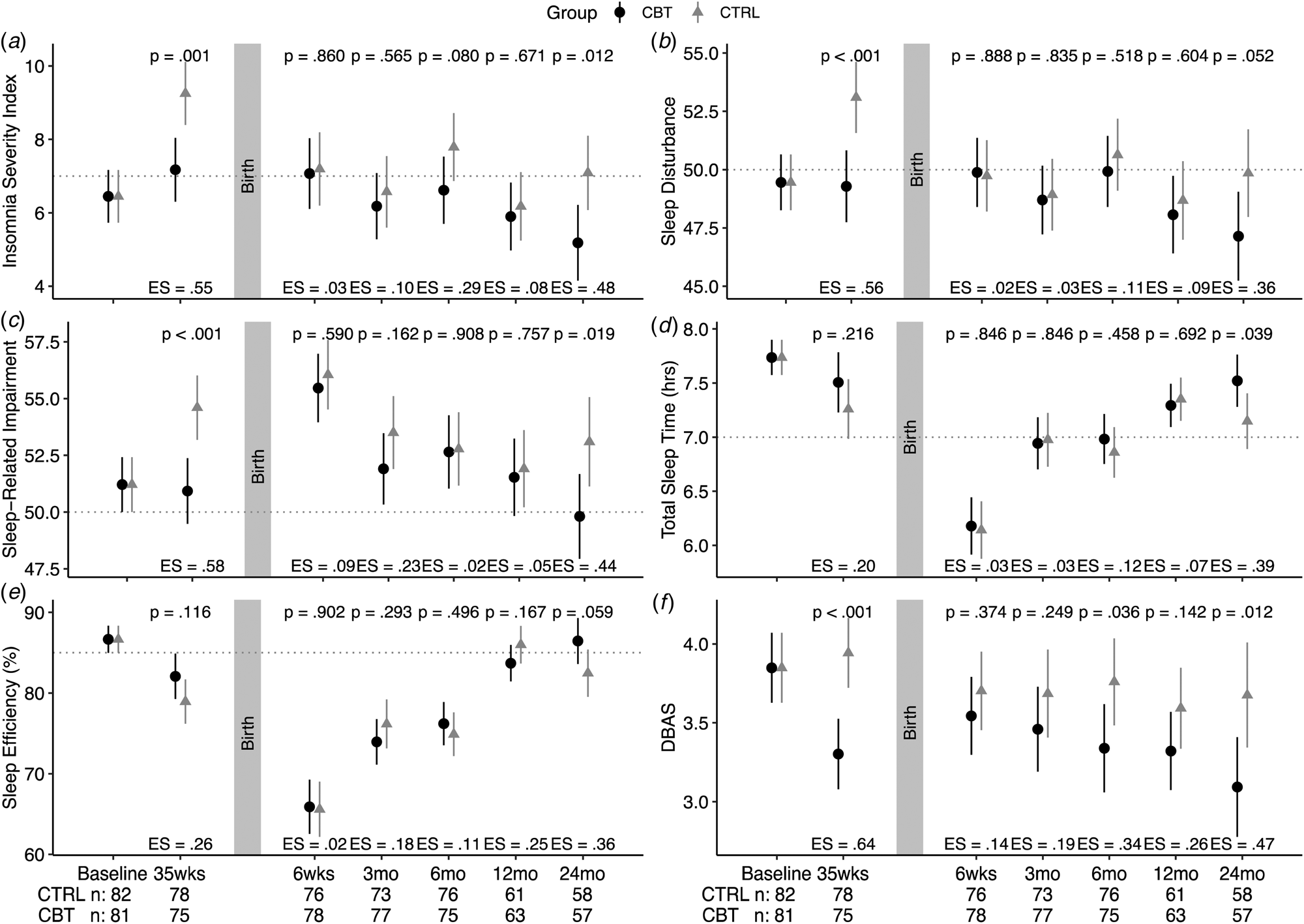
Fig. 2. Model estimated means and 95% confidence interval for sleep-related measures in the intention-to-treat sample.
Note. See online Supplementary Table S1 for numeric summary. All models adjusted for baseline levels of the outcome. ES, effect size; CBT, cognitive behavioural therapy condition; CTRL, active control condition; DBAS, Dysfunctional Beliefs and Attitudes about Sleep Scale.
Secondary outcomes
At the pregnancy endpoint, the CBT condition had significantly lower sleep-related impairment (p < 0.001, ES = 0.58) and DBAS (p < 0.001, ES = 0.64). From T1 to T2, the percentage of participants meeting insomnia diagnostic criteria in the CBT condition reduced from 18.5% to 13.1%, whilst that of the CTRL condition increased from 13.4% to 26.2% (p < 0.001; online Supplementary Table S2). The two conditions did not differ significantly on TST (p = 0.23) or SE (p = 0.12).
During the first postpartum year (T4–T7), the two conditions were comparable on most measures, with the only significant difference being the CBT condition having a lower score on the DBAS at T6 (p = 0.036, ES = 0.34). At 2-year postpartum (T8), however, the CBT condition was lower on the ISI (p = 0.012, ES = 0.48), sleep disturbance (p = 0.052, ES = 0.36), sleep-related impairment (p = 0.019, ES = 0.44) and DBAS (p = 0.012, ES = 0.47), and had longer TST (p = 0.039, ES = 0.39) and higher SE (p = 0.059, ES = 0.36). Details are in Fig. 2 and online Supplementary Table S1. The rates of insomnia diagnosis were low and comparable between conditions during all postpartum time points (online Supplementary Table S2).
Participants from the two conditions reported comparable levels of depression and anxiety symptoms across all measurement time points (see online Supplementary Table S1), except that CBT condition had higher depressive symptoms at T6 compared to CTRL (p = 0.046, ES = 0.33).
Exploratory analyses
Findings on a subgroup of 56 (34.4% of the randomised sample) participants with elevated baseline ISI (>7) are in online Supplementary Tables S2 and S3 and Fig. S1. Results were similar to those of the overall sample, but effect sizes were substantially higher in this subgroup. Participants who received CBT (compared to CTRL): (a) scored lower on the ISI at all post-baseline time points except T4 (1.5 months postpartum), with effect sizes ranging 0.62–0.97; (b) had lower sleep-related impairment at T5 (ES = 0.63), lower sleep disturbance (ES = 0.67) at T7 and lower DBAS at T5 (ES = 0.64) and T6 (ES = 0.86); (c) scored significantly better on all sleep outcomes at T8, with much larger effect sizes (0.75–1.21) compared to those of the overall sample (0.36–0.48). The two intervention conditions reported comparable levels of depression and anxiety symptoms across all measurement time points.
Discussion
To our knowledge, this is the first RCT to evaluate the short-, medium- and long-term efficacy of a non-pharmacological sleep intervention in the perinatal periods, a time when new parents are particularly vulnerable to sleep problems. Compared to receiving an attention- and time-matched control, receiving a cognitive behavioural sleep intervention was associated with lower symptoms of insomnia, sleep disturbance and sleep-related impairment during late pregnancy. Across the first postpartum year, CBT did not have benefits to sleep above that of the control condition; at 2 years postpartum, however, participants who received CBT had better scores on all sleep outcomes examined. The subgroup of participants who had elevated insomnia symptoms at baseline experienced substantially more benefits if they received CBT (v. CTRL): in addition to better sleep during late pregnancy and 2-year postpartum, they also had lower insomnia symptoms during the first postpartum year.
Feasibility and acceptability
The intervention combining digital and telephone delivery was feasible and well accepted. Recruitment data showed that a one-off invitation email reached nearly half of all individuals enrolled in childbirth education, suggesting that this is an effective way to reach new parents in a public perinatal service; this rate would likely be higher had a second reminder invitation been sent. Engagement in CBT was high. Among those who started CBT (n = 78) during pregnancy, only two dropped out before the end of the intervention at 6 months postpartum. Despite ‘time poor’ being a common depiction of the perinatal transition, 82.3% of intervention emails were opened. Satisfaction was also high, with 94.7% reporting satisfied with the intervention they received.
Efficacy during pregnancy
Findings at the pregnancy endpoint add to the small but growing literature that CBT, in various modes of delivery (e.g., in-person, online, telephone), is efficacious in reducing symptoms of insomnia during pregnancy (Felder et al., Reference Felder, Epel, Neuhaus, Krystal and Prather2020; Kalmbach et al., Reference Kalmbach, Cheng, O'Brien, Swanson, Sangha, Sen and Drake2020; Manber et al., Reference Manber, Bei, Simpson, Asarnow, Rangel, Sit and Lyell2019). In the control condition, insomnia symptom severity, its diagnostic prevalence, sleep disturbance and sleep-related impairment all increased substantially from early to late third trimester (T1 baseline to T2); this increase in sleep complaints is well documented in observational studies (Sivertsen et al., Reference Sivertsen, Hysing, Dørheim and Eberhard-Gran2015). The average PROMIS Sleep Disturbance and sleep-related impairment scores at T2 for the control condition were elevated and were at 63rd and 68th percentile of the population norm.
In contrast, in the CBT condition, these sleep domains remained stable or improved across the same time frame. Thus, CBT was efficacious in buffering against the natural increase in sleep complaints during late pregnancy. Moreover, the average PROMIS Sleep Disturbance and sleep-related impairment scores at T2 did not differ significantly from population average (scores of 50), as indicated in their 95% confidence intervals including 50. In other words, whereas sleep and related impairment worsened for participants in the control condition, these outcomes normalised for those in the CBT condition to levels comparable to that experienced in the general non-pregnant populations.
Efficacy during postpartum
CBT did not show benefits in sleep outcomes in the overall sample during the first postpartum year (i.e., 1.5, 3, 6 and 12 months postpartum). This is consistent with similar null findings in two other RCTs that used in-person CBT and followed up until 3 (Sweeney et al., Reference Sweeney, Signal and Babbage2020) and 10 (Kempler et al., Reference Kempler, Sharpe, Marshall and Bartlett2020) months postpartum, respectively. One likely explanation is that significant sleep disruption (about 50–90 min less sleep per night over the first six postpartum months, compared to the third trimester) masked CBT's effects. A large longitudinal study showed that although sleep stabilised in 66% of infants from 6 months onward, 34% reported having seven nights of awakenings per week at 6 months, dropping to two nights per week at 15 months, and to one night per week by 2 years (Weinraub et al., Reference Weinraub, Bender, Friedman, Susman, Knoke, Bradley and Williams2012). Indeed, in this study, it was at 2 years postpartum (but not earlier), when infants were likely sleeping through most nights, that therapeutic benefits of CBT became apparent.
In this study, about a third of the sample had elevated symptoms of insomnia at baseline. Although the average ISI of this subgroup (11.70) is somewhat lower than ~15.5 reported in individuals with confirmed diagnosis of prenatal insomnia disorder (Manber et al., Reference Manber, Bei, Simpson, Asarnow, Rangel, Sit and Lyell2019), they scored at 78th percentile of the population norm on the PROMIS for both sleep disturbance and sleep-related impairments. The benefits of CBT after childbirth did not become apparent until 2 years postpartum in the overall sample; this subgroup with elevated symptoms at baseline, however, had lower symptoms of insomnia at four of the five postpartum time points if they received CBT (v. CTRL). Further, treatment effect sizes were substantially larger in these participants compared to the overall sample. In the CTRL condition however, average scores of insomnia symptom severity in this subgroup hovered around 9–10, consistently above the subclinical threshold of 7 for the ISI throughout all postpartum time points. This suggests that, if not addressed, insomnia symptoms presented during pregnancy are likely to persist and likely exacerbate the natural worsening of sleep that is caused by nocturnal infant care; on the other hand, addressing sleep complaints in these vulnerable individuals could lead to sustained benefits during the first two postpartum years.
In further exploratory analyses excluding participants with baseline ISI > 7, we found that at the pregnancy endpoint, effect sizes for sleep outcomes in this low-complaint group were somewhat smaller than, but mostly comparable to, the overall sample (e.g. 0.38 v. 0.55 for ISI, 0.50 v. 0.56 for SD). During postpartum time points, effect sizes for sleep outcomes in the low-complaint group, including at 2-year postpartum, appeared to be small, with effect sizes ranging 0.14–0.21. It is possible that participants with low baseline sleep complaint contributed to null findings for postpartum time points, whilst participants with high sleep complaint contributed to the long-term benefits in the overall sample. However, these exploratory findings need to be interpreted with caution as they were post hoc and under-powered.
Other findings
Unhelpful thoughts and beliefs about sleep are widely accepted to be a perpetuating factor for insomnia and are a therapeutic target of CBT (Spielman, Caruso, & Glovinsky, Reference Spielman, Caruso and Glovinsky1987). In this study, overall endorsement of these thoughts and beliefs was relatively low (3–4 out of 10), and variations over time small. The CBT condition had an average of 14.3% and 19.7% reduction in endorsement at T2 and T8, respectively, whilst endorsement in the control condition remained comparable to baseline over time. It is unclear whether such small reduction in unhelpful thoughts and beliefs about sleep on an already low level of endorsement is clinically meaningful.
To the best of our knowledge, this is the first study that carried out gold-standard structured interviews to assess insomnia disorder diagnostic status longitudinally across the perinatal transition from late pregnancy to 2 years postpartum. The rate of DSM-5 Insomnia Disorder (less the duration criteria) was 16.0% at third trimester baseline in this community sample, higher than the 6–10% reported in the general population (American Psychiatric Association, 2013), but substantially lower than the >60% previously estimated in pregnancy based on questionnaires (Sivertsen et al., Reference Sivertsen, Hysing, Dørheim and Eberhard-Gran2015). Similarly, insomnia disorder rate in the CTRL condition is around 10% during the postpartum time points in this study, much lower compared to previous estimates of 40–60% (Sivertsen et al., Reference Sivertsen, Hysing, Dørheim and Eberhard-Gran2015) based on questionnaire. This difference is unlikely due to lower sleep complaints, as the baseline average ISI score in this population is comparable to that from other community samples in pregnancy (Kempler et al., Reference Kempler, Sharpe, Marshall and Bartlett2020; Manber et al., Reference Manber, Steidtmann, Chambers, Ganger, Horwitz and Connelly2013). But rather, lower rates of insomnia disorder in this study are likely due to other studies using self-report rating scale, whilst this study using structured clinical interview. During the interview, we were able to carefully differentiate sleep disruption (e.g., due to discomfort, infant care) from insomnia, the latter requires sleep problems to persist despite adequate sleep opportunity and sleep conducive environment. This criterion is important in diagnosing insomnia in the perinatal periods, as both sleep disruption and insomnia could result in high scores on a rating scale, but those with sleep disruption should not be misdiagnosed as having insomnia.
The null findings on mood outcomes are consistent with two other recent RCTs in the perinatal periods, one in individuals with insomnia disorder (Manber et al., Reference Manber, Bei, Simpson, Asarnow, Rangel, Sit and Lyell2019), the other community sample (Kempler et al., Reference Kempler, Sharpe, Marshall and Bartlett2020). It is important to note that despite strong associations between sleep complaints and perinatal mood disturbance, currently there is a lack of well-powered RCTs on whether sleep interventions per se improve perinatal mood; this and the other two RCTs cited here were powered for sleep outcomes and not mood. Null findings in this study may be due to the current sample presenting with low levels of mood symptoms, with both the means of PROMIS Depression and Anxiety under 50 (population mean).
Limitations
First, the study did not include objective measures of sleep, and hence does not inform intervention effects on objective sleep. Although some versions of PROMIS physical and mental health short forms were recently validated in the perinatal periods (Slavin, Gamble, Creedy, Fenwick, & Pallant, Reference Slavin, Gamble, Creedy, Fenwick and Pallant2019), the specific short forms used in this study were not. Future scale validation effort is needed for assessing unique sleep and mental health challenges during the perinatal transition. In addition, the following sample characteristics limit the generalisability of findings: (a) all participants were nulliparous; (b) recruitment was carried out via Childbirth Education, where individuals were more likely to be open to health information; (c) the sample was highly educated, predominantly white and mostly in stable relationships. Our previous RCT for prenatal insomnia disorder showed that CBT-I was well received by an ethnically and socioeconomically diverse sample that was 38% Hispanic (Manber et al., Reference Manber, Bei, Simpson, Asarnow, Rangel, Sit and Lyell2019). Future research in diverse socioeconomic and cultural settings is much needed. Findings also may not generalise to individuals with severe psychiatric and physical health conditions (6.3% of screened sample), who were excluded in the study because their sleep was affected by confounding factors that were unlikely to alter with the intervention. Where circumstances allow, these individuals may benefit from concurrent treatments for sleep and these co-existing conditions. In individuals with comorbid major depressive and insomnia disorders, CBT-I is feasible and efficacious (Carney et al., Reference Carney, Edinger, Kuchibhatla, Lachowski, Bogouslavsky, Krystal and Shapiro2017; Manber et al., Reference Manber, Buysse, Edinger, Krystal, Luther, Wisniewski and Thase2016), and improving sleep during the early phase of the treatment predicted better long-term depression outcome (Bei et al., Reference Bei, Asarnow, Krystal, Edinger, Buysse and Manber2018). Finally, findings may not generalise to countries with different parental leave schemes than Australia.
Clinical implications
This longitudinal RCT showed that a scalable cognitive behavioural sleep intervention, tailored for the perinatal periods, is feasible, acceptable and efficacious in buffering against the natural increase in sleep complaints during the third trimester. Moreover, the intervention had long-term benefits to gestational parents' sleep at 2-year postpartum. Given the high prevalence of sleep disturbances and parents' strong preference for non-pharmacological approaches to improve sleep in the perinatal periods (Sedov, Madsen, Goodman, & Tomfohr-Madsen, Reference Sedov, Madsen, Goodman and Tomfohr-Madsen2019), this scalable intervention holds a potential to reach large numbers of new parents in the community.
There are several considerations in wider dissemination of sleep intervention in perinatal care. First, automated digital content distribution used in this study can be scaled up at low cost and offered to any individual who may be interested in improving sleep during their antenatal visits. Second, clinicians such as midwives and nurses could be trained to deliver the brief one-on-one support for intervention materials. Such individualised support would particularly benefit those who present with symptoms of insomnia during pregnancy, who stand to benefit the most from this intervention. Finally, further implementation and health economics evaluation is needed to further determine the barriers, facilitators and cost-effectiveness of incorporating such a scalable sleep intervention in real-world practice.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291721001860.
Acknowledgements
The authors would like to thank all participants for generously donating their time to this project. We thank Kaye Dyson and Elisabeth Gasparini for supporting recruitment, Drs Allie Peters and Monika Raniti for delivering the sleep intervention, Dr Sarah Meiklejohn for delivering the diet intervention, and (alphabetical) Laura Astbury, Cassandra Fong, Dr Catherine Fulgoni, Anthony Hand, Ashley Lam, Jin Joo Lee, Sarah Samuel, Isabelle Smith, Emma Thompson and Sumedha Verma for assistance in collecting data used in this manuscript. We thank Dr Addie Wootten for coordinating the sleep intervention's use and access of audio materials from Smiling Mind.
Financial support
Data collection was supported by Rob Pierce Grant-in-Aid and Helen Bearpark Scholarship from Australasian Sleep Association, Strategic Grant Scheme from the Faculty of Medicine, Nursing and Health Sciences, Monash University, and the Royal Women's Hospital Foundation. Intervention materials were adapted from those developed via a National Institute of Health R01 grant (NR013662). Bei (APP1140299) and Wiley (APP1178487) are supported by the National Health and Medical Research Council Fellowships, and Pinnington, Quin, Shen by Australian Postgraduate Awards by the Department of Education and Training. The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Conflict of interests
SPAD reports personal fees from Zelda Therapeutics, personal fees from Jazz Pharmaceuticals, outside the submitted work; this is unrelated to the work carried out in this manuscript. RM received royalties from Guilford Press and New Harbinger for books on insomnia treatment; RM is also a paid Deputy Editor in Chief of the journal SLEEP; these are unrelated to the work carried out in this manuscript. Other authors have nothing to disclose.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Ethical approvals were obtained from the Royal Women's Hospital and Monash University Human Research Ethics Committee.





