



Introduction
Tympanic membrane retractions are an unwanted consequence of sharp variations in middle-ear pressure.Reference Sadé, Avraham and Brown1 This is mainly attributed to the reduced functionality of the Eustachian tube's pressure equalisation.Reference Holmquist, Renvall and Svendsen2,Reference Borgstein, Gerritsma and Bruce3 Retractions of the tympanic membrane follow progressive changes, from simple retractions to retraction pockets, to retraction pockets with cholesteatoma.Reference Sadé, Avraham and Brown1,Reference Holmquist, Renvall and Svendsen2 Tympanic membrane retractions are one of the most significant causes of conductive hearing loss, particularly as a result of ossicular erosion.
Sadé et al. divided pars tensa retractions into four grades (grade I to grade IV).Reference Sadé, Avraham and Brown1 However, the significance of ossicular necrosis or association with cholesteatoma was not considered in their study. Little emphasis was given to categorising the pars tensa retractions based on the ossicular status and association with cholesteatoma. Despite the proposal and use of several staging systems, ratification of the same with repeated assessments has been sparse.Reference Borgstein, Gerritsma and Bruce3 Interpretation of the grading system may be prone to variability given subjective differences in terms of the extent of ossicular erosion or depth of tympanic membrane retraction.Reference James, Papsin, Ramsden and Bailie4,Reference Borgstein, Gerritsma, Wieringa and Bruce5
In addition, there is often a progressive change from simple pars tensa retractions to pars tensa retractions with cholesteatoma.Reference Sadé and Ar6,Reference Sadé, Amos, Ludman and Wright7 Pars tensa retractions also progress to ossicular necrosis, which is a leading cause for conductive hearing loss.Reference Sadé, Amos, Ludman and Wright7 The Sadé grading system does not take into account the ossicular necrosis or the association of cholesteatoma with the retractions.Reference Pothier8–Reference Yoon, Schachern, Paparella and Aeppli10 Subjective differences in the interpretation of different grading systems of pars tensa retraction, in terms of the extent of ossicular erosion and depth of tympanic membrane retraction, results in inconsistency.Reference Borgstein, Gerritsma and Bruce3,Reference Sharp and Robinson11,Reference Srinivasan, Banhegyi, O'Sullivan and Sherman12 Erosion of the ossicles as a complication of pars tensa retraction is frequently observed, but rarely discussed.Reference Fuh-Cherng, Ming-Hsui and Brown13,Reference Dornelles, Costa, Meurer and Schweiger14
In our decades of experience as a tertiary otological centre, we, like others, have found that the occurrence of ossicular erosion and cholesteatoma is not uncommon. We have discovered that, in addressing these pars tensa retractions, erosion and cholesteatoma should be given importance when categorising the tympanic membrane retractions. We have found that erosion and cholesteatoma play important roles in the diminution of hearing and in mapping out future management. Thus, this retrospective study was assembled to illustrate our classification of pars tensa retractions, which is more precise than previous systems.
Our centre makes use of oto-endoscopy to determine the depth and extension of retraction pockets, and we use photo-documentation to better refer to each patient's retraction. For years, we found that direct line-of-sight microscopy or otoscopy could not capture the depth and extent of retraction pockets.
Materials and methods
This retrospective study was reviewed by Vijaya ENT Care Centre's Ethics Committee and received approval (protocol number: 2021-23).
Evaluations
A retrospective study was carried out on 200 ears of 170 patients whose pars tensa retractions had been documented at a tertiary otological referral centre in India over a duration of six years, from October 2015 through September 2020. All patients underwent detailed clinical examination with oto-endoscopic photo-documentation. The Valsalva manoeuvre was performed and the ability to lift the pars tensa retraction off of the promontory was determined, in order to assess tympanic membrane adherence to the promontory. Audiological evaluation of all patients was carried out, and the pure tone average (PTA) of 0.5, 1, 2 and 4 kHz was recorded. All patients were classified using the new classification system proposed in this study, ranging from grade 1 to grade 5.
Patient exclusions
Only patients who had isolated pars tensa retraction, and who underwent oto-endoscopic photo-documentation, the Valsalva manoeuvre, and audiometric examination were included in the study. Patients aged under 10 years were not included because of inconsistencies in performing the Valsalva manoeuvre properly. Patients with a dual pathology involving both pars tensa retractions and pars flaccida retractions were excluded. Patients who had undergone any previous ear surgery were also excluded.
Developed classification system
The classification system, developed from observations between 2015 and 2020, is presented in Figure 1.
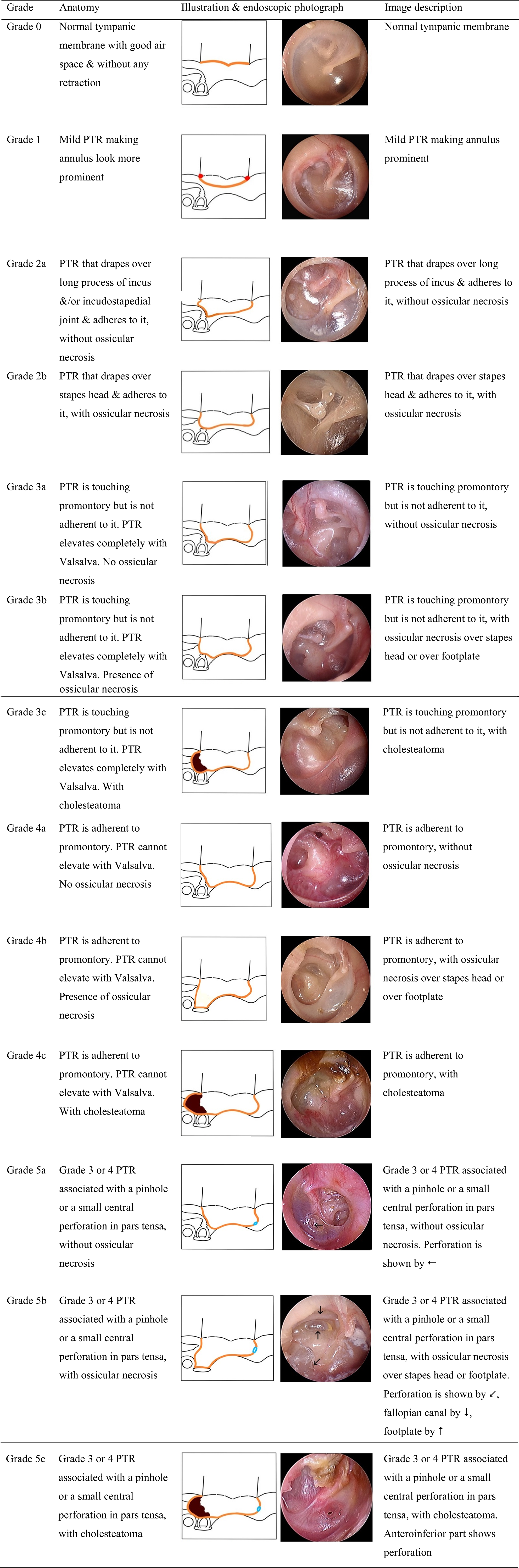
Figure 1. Classification system of pars tensa retraction (PTR).
Results
These results concern the retrospective classification of patients.
Patient findings
The study was conducted by reviewing the medical records of patients who met the inclusion and exclusion criteria for isolated pars tensa retractions. A total of 170 patients (64 females and 106 males) and a total of 200 ears with pars tensa retractions were identified. Patients aged under 10 years were not included in the study.
In no instance was the attribution of pars tensa retraction grade ambiguous or difficult to determine. Table 1 shows that the prevalence of the pars tensa retractions decreased with age. The maximal number of pars tensa retractions were seen in ages 21–30 years (31 per cent), followed by ages 11–20 years (24 per cent). The least number of cases were seen in patients aged 61–70 years (3 per cent).
Table 1. Distribution of ages in patients with pars tensa retractions

PTR = pars tensa retraction
Prevalence and hearing function
Table 2 shows the prevalence of each pars tensa retraction grade. Findings of tympanic membranes that were less retracted and less adherent, with less ossicular erosion, were more common than findings of more anatomical disruption. Each progressively severe grade was less prevalent than the previous grade. The least retracted grade 1 was present in 19 per cent of the pars tensa retractions, while grades 5a, 5b and 5c, with retraction, adherence and erosion, were present in 4 per cent, 5 per cent and 3 per cent, respectively.
Table 2. Distribution of ears according to pars tensa retraction grade

PTR = pars tensa retraction
Table 3 shows the deterioration of PTA with increased pars tensa retraction grade. The PTAs ranged from minimal hearing loss in the low grades up to 62.4 dB in grade 5 cases. Each grade showed worse PTAs in subcategory ‘b’ compared to subcategory ‘a’. However, in each grade, the subcategory ‘c’, which indicated a cholesteatoma, showed PTAs between subcategories ‘a’ and ‘b’; in other words, the presence of cholesteatoma improved the PTA, as seen in cases of cholesteatoma bridge.
Table 3. PTA of ears according to pars tensa retraction grade

PTA = pure tone average; PTR = pars tensa retraction
Discussion
This classification system for pars tensa retractions was developed and confirmed by a review of the findings in 170 patients with 200 pars tensa retractions. All patients’ findings allowed attribution of one of the grades without exception. The temporal progression of pars tensa retraction grade and the temporal progression of anatomical disruption seem to mirror each other, as seen by the distribution of grades and PTAs of the ears with pars tensa retractions. Specifically, the numbers of ears in each grade diminish with the severity of the pars tensa retraction grade, and the severity of hearing loss increases with each grade. These two correlations strongly suggest that the tympanic membrane passes through gradually worsening retraction, progressing to promontory adhesion and ossicular erosion. In addition, the anatomical disruption is paralleled by the deterioration of sound transmission, as demonstrated by the worsening PTAs with increasing grade.
The present study, with a level of evidence of 5, categorises pars tensa retraction into six grades (grade 0 to grade 5), and prioritises ossicular necrosis and the association with cholesteatoma in different stages individually. This approach addresses some limitations of previous pars tensa retraction classification schemes.
Sadé et al., in 1981, studied tympanic membrane atelectasis and retraction pocket dynamics, and classified pars tensa retractions into four different grades (grade I to grade IV); this is the most widely used grading system for pars tensa retractions to date.Reference Sadé, Avraham and Brown1 Grade I reflected a slight retraction of the tympanic membrane making the annulus look more prominent. Grade II indicated the tympanic membrane touching the incus or stapes. Grade III represented the tympanic membrane touching the promontory, but not adherent to it. Grade IV indicated a tympanic membrane adherent to the promontory. In their study, although the sample size was 308 ears, 150 (48.7 per cent) were of grades I and II. Of these 150 ears, 94 required no intervention. Eighty ears (25.9 per cent) had grade III retraction, of which seven required no intervention. Sixty-nine ears (22.4 per cent) had grade IV retraction, and 25 of these required no intervention. No emphasis was given to ossicular destruction or the association with cholesteatoma in their study. Our study incorporates erosion and cholesteatoma.
In a study conducted by James et al. on the endoscopic evaluation of a tympanic membrane retraction staging system, 245 ears were examined by 6 different observers.Reference James, Papsin, Ramsden and Bailie4 A total of 108 (44 per cent) tympanic membranes had pars tensa retractions or pars flaccida retractions, and 41 tympanic membranes were excluded for having a perforation.Reference James, Papsin, Ramsden and Bailie4 Of the ears, 137 (56 per cent) had no signs of retraction. The authors classified pars tensa retractions into seven grades. Grade 0 was a normal tympanic membrane. Grade 1a was a pars tensa retraction not in contact with any middle-ear structures, and grade 1b involved the pars tensa retraction touching the promontory. Grade 2a was a pars tensa retraction touching the incus, and grade 2b was a pars tensa retraction enveloping the incus. Grade 3a was a pars tensa retraction eroding the incus partially, and grade 3b was a pars tensa retraction eroding the incus completely. Grade 4 was a pars tensa retraction disappearing out of sight. Grade 5 included keratin accumulation medial to the annulus. Grade 6 involved granulation tissue at the pars tensa retraction. Grade 7 was categorised as cholesteatoma. Their study took ossicular erosion and cholesteatoma into account, but categorised them into separate categories and did not parse them into the appropriate grades of retraction. Our study parses erosion and cholesteatoma by pars tensa retraction grade.
Borgstein et al., in 2007, proposed the Erasmus atelectasis classification for pars tensa retractions.Reference Borgstein, Gerritsma, Wieringa and Bruce5 They classified pars tensa retractions according to five stages. Stage I was an atrophic, non-adherent tympanic membrane. Stage II was a tympanic membrane adherent to the promontory. Stage III was a tympanic membrane adherent to the incus and/or stapes. Stage IV was a tympanic membrane adherent to the ossicles with pars tensa retraction, but without cholesteatoma. Stage V was pars tensa retraction with cholesteatoma and/or breakthrough. Their study lacked emphasis on adult patients and ossicular status. In addition, the association with cholesteatoma in different stages of retraction was not addressed. Our study incorporates adult patients and addresses erosion.
• Previous classification systems of pars tensa retractions (which focused on paediatric patients) have not consistently incorporated, or have segregated, ossicular erosion and presence of cholesteatoma
• Hence, these systems do not easily lend themselves to the array of pars tensa retraction patients and to future surgical management planning
• This retrospective study comprised patients with isolated pars tensa retractions graded using oto-endoscopic photo-documentation, Valsalva manoeuvre and pure tone average findings
• Pure tone average was progressively worse with the higher grades, with ossicular necrosis and cholesteatoma, compared to an intact ossicular chain
• This classification system could accommodate all pars tensa retractions; grade distribution was based on ossicular status and presence of cholesteatoma
• The classification system is a more applicable and functionally based system than previous alternatives
Regarding weaknesses of the current study, the prevalence of each grade of pars tensa retraction could be determined for the patients who presented to the tertiary care centre, but cannot be known for the population at large. This study could be improved by following each pars tensa retraction over time to see if each retraction did indeed progress through each successive grade of pathology. However, such a management plan would likely not be chosen by patients presenting for medical intervention, and may pose ethical problems. Finally, we cannot explain the male predominance in the patients who presented to our centre.
This study has demonstrated a logical classification system that can be employed through oto-endoscopic visualisation and determining associations with corresponding hearing loss. Our future work will focus on the differential management of each retraction type and the usual outcomes of the differential management.
Conclusion
The classification system of pars tensa retractions developed in this study incorporates the progression of pars tensa retractions and ossicular destruction, and the association with cholesteatoma. It can aid in predicting future hearing deficits and in mapping out the management plan for each grade of retraction.
Competing interests
None declared.




