Introduction
Most psychological interventions that are currently used to treat patients with schizophrenia-spectrum disorders, such as psychoeducation, cognitive behavioral therapy (CBT), and cognitive interventions show only moderate beneficial effects on psychotic symptoms (Lincoln & Pedersen, Reference Lincoln and Pedersen2019). This is evidenced through both low effect sizes of each of them and small differences between them with trivial clinical significance (Turner, van der Gaag, Karyotaki, & Cuijpers, Reference Turner, van der Gaag, Karyotaki and Cuijpers2014). Other outcomes that are closely related to the patients' everyday life, such as quality of life (QoL), may therefore represent a suitable candidate for evaluating treatment success (Awad & Voruganti, Reference Awad and Voruganti2012). Nowadays, QoL is understood as a multidimensional construct which encompasses different indicators. Objective QoL refers to observable indicators such as finance, housing, or number of friends (Katschnig, Reference Katschnig2006) whilst subjective QoL refers to an individual's appraisal of several life domains such as relationship quality, accommodation, or safety (Lehman, Reference Lehman1988). The person's subjective perception that is specifically related to their health status and its consequences is defined as health-related QoL (Patrick & Chiang, Reference Patrick and Chiang2000).
So far, one prior meta-analysis aimed at assessing the intervention effectiveness for schizophrenia-spectrum disorders on QoL (Valiente, Espinosa, Trucharte, Nieto, & Martinez-Prado, Reference Valiente, Espinosa, Trucharte, Nieto and Martinez-Prado2019). However, the evidential value of this prior meta-analytical account is limited due to (i) an insufficient identification of eligible studies as a result of a suboptimal search strategy (i.e. limited databases, broadly defined search terms), as well as (ii) the unobserved heterogeneity that likely emerged from mixing both predicting (in terms of differences in intervention type and composition, as well as of inclusion of several different mental diagnoses) and outcome variables (in terms of subjective v. objective QoL assessments). The latter point yields well-known effect-distorting mechanisms that are rooted in the apples-and-oranges problem [see Petkari, Reference Petkari2023, for a detailed review].
To be able to yield meaningful findings in terms of intervention effectiveness, the following points need to be taken into consideration. First, to guide clinical practice the effect sizes of standalone psychological interventions should be calculated separately (Mueser, Deavers, Penn, & Cassisi, Reference Mueser, Deavers, Penn and Cassisi2013), without admixture with multicomponent care programs (i.e. medication, case management, assertive community treatment, vocational services), or peer-led interventions. Second, QoL differs between people with schizophrenia and other mental disorders (Ådnanes et al., Reference Ådnanes, Kalseth, Ose, Ruud, Rugkåsa and Puntis2019; Berghöfer, Martin, Hense, Weinmann, & Roll, Reference Berghöfer, Martin, Hense, Weinmann and Roll2020; Petkari & Priebe, Reference Petkari and Priebe2023) suggesting differences in treatment effectiveness. Third, the effects on objective and subjective QoL indicators should be calculated separately, because in patients with schizophrenia they seem to be at best moderately associated with each other (Hayhurst, Massie, Dunn, Lewis, & Drake, Reference Hayhurst, Massie, Dunn, Lewis and Drake2014; Renwick et al., Reference Renwick, Drennan, Sheridan, Owens, Lyne, O'Donoghue and Clarke2017) and the two QoL indicators show different relationships with other factors. For example, negative symptoms (Eack & Newhill, Reference Eack and Newhill2007) and functioning (Nevarez-Flores et al., Reference Nevarez-Flores, Sanderson, Breslin, Carr, Morgan and Neil2019) show small associations with subjective QoL but large associations with objective QoL, whereas service satisfaction (Petkari & Pietschnig, Reference Petkari and Pietschnig2015) shows moderate associations with subjective but no associations with objective QoL.
Therefore, the aims of the present meta-analysis are (i) to examine the effects of the psychological interventions on different QoL indicators (objective and subjective) in patients with schizophrenia-spectrum disorders; (ii) to determine which interventions are more effective (psychoeducation v. CBT v. cognitive v. combination of several types v. other psychological interventions such as psychodynamic, systemic, etc.); and (iii) to identify moderating variables of intervention effectiveness (i.e. duration of intervention; modality: group v. individual v. both; illness length; service context: outpatients v. inpatients v. both; and treatment of comparison group: TAU v. other psychological intervention v. non therapeutic intervention).
Methods
This meta-analysis was registered at PROSPERO (CRD42022335055) and was prepared according to the PRISMA guidelines (Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow and Moher2021).
Literature search
The following databases were searched for documents until January 2023: Proquest, PUBMED/MEDLINE, PsycINFO, Web of Science, Scopus, and the Cochrane Library. Moreover, we hand-searched references of relevant articles and previous meta-analyses. Hits were not restricted in terms of language or publication period. The search included a combination of keywords related to the population, intervention types, design of studies and outcomes, and was based on Abstract, Title, and Keywords (wherever available). The specific search string was: (‘Psychosis’ OR ‘Psychoses’ OR ‘Psychotic’ OR ‘severe mental illness’ OR ‘schizophrenia’) AND (‘Quality of Life’ OR ‘QoL’) AND (‘intervention’ OR ‘therapy’ OR ‘training’) AND (‘Randomised’ OR ‘Randomized’ OR ‘RCT’).
Inclusion criteria
To be eligible for inclusion, primary studies needed to have (i) used an RCT design, (ii) studied adult patients suffering from schizophrenia-spectrum disorders (i.e. schizophrenia, schizoaffective, schizophreniform, delusional, as established by known diagnostic classification criteria (i.e. DSM, ICD) or clinical records; studies including participants with other diagnoses such as bipolar, depression, or other severe mental illnesses, and patients with substance abuse difficulties were excluded), (iii) included patients attending inpatient or outpatient clinical settings, (iv) examined the effectiveness of psychological interventions (i.e. theory-driven, delivered by a trained clinician) targeting QoL (or assessing it as an outcome), (v) included a control group of patients receiving treatment as usual (TAU: i.e. rehabilitation services, being on the waiting list for the treatment under study; receiving any other psychological intervention, or receiving non-therapeutic interventions matched for the study purposes such as computer games or befriending; we excluded multicomponent rehabilitation programs from which the intervention's unique effect could not be isolated, interventions targeting physical/body health [i.e. exercise, weight control, yoga/tai chi], vocational rehabilitation interventions, and interventions not including a therapist [i.e. virtual/mobile applications], (vi) used a standardized instrument for QoL assessment (i.e. objective, subjective/health-related), (vii) reported sufficient statistical parameters to allow a calculation of effect sizes or provided them upon request from the corresponding authors, and (viii) not reported duplicates of data that had already been published elsewhere.
Screening and data extraction
One researcher (EP) performed the database searches, merged results, and removed duplicates. Two researchers (EN, EP) independently screened the search output based on Titles and Abstracts twice and then accessed the potentially eligible article full texts. The following information was coded from primary studies: study details: title, author, publication year, location; study design: duration, measured outcomes, follow-up period; participant demographics: age, sex, education; setting: outpatients v. inpatients v. both; sample size for treatment and control arms; diagnoses (% of patients with schizophrenia); mean illness length; medication (in Clorpromazine-CPZ equivalents/day); intervention characteristics: duration, type, modality (group v. individual v. both interventions); control group intervention/condition: TAU v. other intervention v. other non-therapeutic intervention; outcomes: QoL indicator and measure; statistical parameters: means, standard deviations, sample sizes for QoL.
The interventions were grouped as follows, based on their content as described in the primary studies:
(1) Psychoeducation: interventions focusing on psychoeducation/information provision for the patients only, or together with family members
(2) Cognitive: interventions including cognitive training, remediation, metacognitive techniques
(3) CBT: interventions based on cognitive behavioral components
(4) Combination: interventions based on components of several approaches (i.e. combining psychoeducation with CBT; cognitive and problem-solving, etc.)
(5) Other: interventions not fitting the previous categories, including third-generation interventions (i.e. mindfulness, mentalization), art therapy, solution-focused, etc. Discrepancies were resolved through discussion with a third independent researcher (SP). Eight corresponding authors were contacted and two provided missing information for eligible primary studies. A PRISMA flow-chart of study inclusion is available from online Supplementary Fig S1.
Outcomes and quality assessment
We calculated RCT-based changes in QoL indicators between treatment and control groups using the Hedges g metric (i.e. representing small sample-corrected standardized mean differences) as outcome variables. In cases where more than one effect size could be calculated (i.e. due to availability of multiple QoL indicators, treatment groups, or control groups), we included all effect sizes in our analyses and accounted for the resulting data dependencies by using a multilevel approach.
For our two-level multiverse analyses we (i) averaged effect sizes wherever several QoL subscale values were reported, (ii) preferred comparisons with more complex interventions (i.e. combining psychoeducation with CBT) wherever multiple treatment groups were reported, and (iii) preferred comparisons with control groups that had received treatment as usual in cases where multiple control groups were reported.
In all eligible primary studies, QoL was measured through standardized instruments for objective (i.e. QLS), subjective (i.e. MANSA; LQOLP) and health-related (i.e. WHO-QoL) indicators. Subjective and health-related indicators were analyzed within a common category, given the subjective self-reported nature of the instruments.
Study quality was assessed twice by two independent researchers (EN, EP) using the Effective Public Health Practice Project Quality Assessment Tool (EPHPP; Thomas, Ciliska, Dobbins, & Micucci, Reference Thomas, Ciliska, Dobbins and Micucci2004). Studies were rated based on study design, blinding, confounders, instruments psychometric characteristics, and withdrawals/dropouts (see online Supplementary Table S1 for details).
Statistical analyses
We ran all our analyses separately for effect sizes based on objective and subjective (including health-related) QoL. First, we synthesized effect sizes by means of a three-level model to account for within-studies effect size dependencies. To this end, we weighted effect sizes by standard errors (smaller standard errors indicating higher precision and therefore larger weights of studies) using maximum likelihood estimation in random-effects models.
Second, we calculated subgroup effects according to different interventions in the treatment groups (i.e. intervention type: psychoeducation v. CBT v. cognitive v. combination of several types v. other psychological interventions such as psychodynamic, systemic, etc.). Because of comparatively low within-subgroup effect size numbers, nominal statistical significance testing of between-subgroup effect differences was deemed unpractical to evaluate effect differences due to low power, but we provide 95% confidence intervals to allow readers to evaluate the amount of overlap.
Third, we ran a series of eight single precision-weighted mixed-effects multilevel meta-regressions (predictors: mean age; schooling years; percentage of women within sample; illness duration; mean medication [CPZ] intake; percentage of patients with schizophrenia within sample; patient service: inpatients v. outpatients v. mixed; intervention modality: individual v. group v. both) for each outcome variable. We used single regressions instead of multiple models because of the expectable study attrition due to missing values for individual predictors. Categorical variables were dummy-coded prior to data analysis. In supplemental analyses, we investigated influences of differences between treatment and control groups in perceived symptoms and functioning on both QoL types.
We interpreted effect sizes according to the well-established thresholds of Cohen (Reference Cohen2013), assuming absolute gs = 0.2, 0.5, and 0.8 to represent the lower thresholds of small, moderate, and large effects, respectively. All analyses were performed in the open source software environment R 4.2.0 (R Core Team, 2022) by means of the packages metafor (Viechtbauer, Reference Viechtbauer2010) and robumeta (Fisher, Tipton, & Zhipeng, Reference Fisher, Tipton and Zhipeng2017).
Dissemination bias
To investigate potentially confounding influences of dissemination bias, we visually inspected funnel plots and used four formal detection methods, namely: Trim and fill analysis, Egger's regression with sandwich estimators, MLMA-based Egger's regression, and a three-parameter selection model (see online Supplementary file S2 for a detailed description).
Multiverse analyses
It has been shown that different (reasonable) ways to specify study inclusion criteria and how to synthesize the resulting effect sizes may yield substantially differing summary effects and consequently effect interpretations (e.g. Pietschnig, Gerdesmann, Zeiler, & Voracek, Reference Pietschnig, Gerdesmann, Zeiler and Voracek2022). On the one hand, different researchers might disagree on an appropriate way to select primary studies that should be synthesized in a meta-analysis (e.g. preferring certain sample characteristics over others). On the other hand, they might disagree on the appropriate analysis approach (e.g. fixed-effect v. random-effects calculation).
In other words, different researchers may adopt differing approaches to conceptualize studies and analyze their data (this is typically referred to as researcher degrees of freedom e.g. Wicherts et al., Reference Wicherts, Veldkamp, Augusteijn, Bakker, van Aert and van Assen2016). Either approach may be equally reasonable, but may yield different results and therefore implications. Assessing the multiverse of different (un)reasonable ways to set up and analyze our data by means of specification curve and combinatorial meta-analysis can therefore inform us about (i) the generalizability of a given phenomenon and (ii) its robustness against the use of differing analytical approaches. In our multiverse analyses, we used two-level instead of multilevel modeling.
Specification Curve. In many meta-analyses, choosing a certain inclusion or analytical approach over another may seem equally reasonable to a given researcher. However, isolated specific (reasonable) data syntheses in conjunction with specific analyses may yield non-salient effects (see, for instance, the highly publicized but apparently flukish finding of larger destructive effects of hurricanes with girl v. boy names in the USA; Jung, Shavitt, Viswanathan, & Hilbe, Reference Jung, Shavitt, Viswanathan and Hilbe2014; see Simonsohn, Simmons, & Nelson, Reference Simonsohn, Simmons and Nelson2015; Voracek, Kossmeier, & Tran, Reference Voracek, Kossmeier and Tran2019 for an overview).
Thus, contrasting evidence of primary and even meta-analytical studies may obscure salient effects that may be masked by their differentiation according to certain study or sample characteristics. In other words, it makes a difference which data are analyzed and how, but there is mostly no equivocal way to determine a single ideal specification. Instead, often there are many ways to reasonably specify study designs and analytical approaches.
Therefore, calculating summary effects according to all possible combinations of reasonable selection and calculation criteria may provide an indication about the generality or specificity of a given effect. In other words, if summary effect sizes are similar in size, regardless of the respective specification, the true effect can be considered to generalize across moderators. But if effect estimates vary substantially across selection criteria or their combinations, this is indicative of effect differentiation.
Combinatorial Meta-Analysis. It can be argued that considering effects of reasonable specifications only may be insufficient to detect influences of moderators (e.g. because relevant moderators have not been identified yet). One way to identify influences of unobserved heterogeneity has been suggested in terms of combinatorial meta-analyses which is typically illustrated by means of GOSH plots (graphical display of study heterogeneity; Olkin, Dahabreh, & Trikalinos, Reference Olkin, Dahabreh and Trikalinos2012).
In this approach, all possible combinations of effect sizes are considered to represent a possible (albeit potentially unreasonable) way to estimate a summary effect. These summary effects are then related to the resulting between-studies heterogeneity of the corresponding summary effect calculation. When effects are stable, summary effect estimates should not show systematic associations with heterogeneity indices. Because the number of possible summary effect estimates (2k–1) typically exceeds the computational power of most computers nowadays (e.g. for subjective QoL, there would be 245 ≈ 35 trillion possibilities to calculate two-level model-based summary effects), we sampled 100 000 combinations at random, following standard procedure (e.g. Pietschnig et al., Reference Pietschnig, Gerdesmann, Zeiler and Voracek2022).
Results
Final sample
In all, we identified sixty independent studies that met our inclusion criteria, comprising k = 89 study effects (ks = 70 and 19 for subjective and objective QoL; Ns = 6254 and 1024, respectively). More than half of the studies were from Europe (k = 37), nine studies were from Asia, five from USA/Canada, four from Australia, three from South America and two from Africa. The majority of the samples comprised only patients with schizophrenia (mean % of schizophrenia diagnosis within samples = 86.38%), with the rest comprising patients with schizophrenia-spectrum disorders (i.e. including schizoaffective, schizophreniform and delusional), that were predominantly male (63.90%), had on average 11.86 school years, and a mean age of 39.02 years. Mean illness duration was 13.94 years (s.d. = 5.22) and administered medication averaged at 536.14 (s.d. = 264.68) CPZ equivalents/day. Characteristics of the included studies are detailed in Table 1.
Table 1. Characteristics of included studiesa

a References provided as online supplementary material (Supplementary File 1).
Study quality
In terms of the quality ratings by means of the EPHPP Quality Assessment Tool (Thomas et al., Reference Thomas, Ciliska, Dobbins and Micucci2004), 32 studies were of strong, 21 of moderate, and 7 studies of weak quality (see online Supplementary Table S1). Global study quality ratings did not significantly predict effect sizes of neither subjective nor objective QoL (ps = 0.373 and 0.783, respectively), thus indicating no systematic influences of study quality on effect sizes.
Interventions and comparators
There were 15 studies with interventions targeting objective QoL. Six of them used cognitive interventions; four of them used CBT, three used a combination of interventions such as the Illness Management and Recovery (IMR), and two used psychoeducation. The interventions were compared with: other non-therapeutic conditions in seven studies (i.e. computer games, non-specific counseling); TAU in five studies; and other interventions in three studies.
For subjective QoL, there were 45 studies focusing on different interventions, with 11 of them using CBT; 12 of them using other intervention types such as systemic, psychodynamic (art therapy), mindfulness, or family therapy; eight using cognitive interventions; eight using interventions combining different elements such as the IMR or the Integrated Psychological Therapy (IPT); and five using psychoeducation. Most of the studies compared the interventions to TAU (k = 31), seven compared them to other interventions, and seven to other non-therapeutic conditions such as befriending or newspaper reading (see Table 1 for details).
Quality of life outcomes
Most of the studies examining interventions focusing on objective QoL included this as a primary outcome (12 out of 15 studies), whereas for subjective QoL this was true for less than half of the studies (26 out of 45), with the rest considering QoL a secondary outcome. All studies assessing objective QoL used the Quality of Life Scale (QLS) (k = 15). Subjective (including health-related) QoL was assessed through a variety of instruments, with the most commonly used being the WHO-QoL (k = 13) and the Manchester Short Assessment of Quality of Life (MANSA) (k = 10) (see Table 1).
Intervention effectiveness on QoL
Our results indicated substantial larger intervention effects of most treatments on objective QoL compared to subjective QoL. Overall, non-trivial and significant, albeit small positive effects of treatments compared to controls were observed for objective QoL (overall g = 0.330; p = 0.026), whilst overall treatment effects on subjective QoL were non-significant and merely trivial (overall g = 0.184; p = 0.118; Table 2).
Table 2. Multilevel meta-analyses of (specific) intervention effectiveness on objective and subjective Quality of Life

This general pattern of results held up for almost all intervention-based multilevel subgroup analyses. For objective QoL, psychoeducation appeared to have the most beneficial intervention effects, yielding a significant large effect (g = 0.909, p = 0.048). CBT-based interventions showed a modest-to-strong (g = 0.653) and cognitive interventions a small, but non-trivial, positive effect (g = 0.241), although both summary effects were nominally non-significant. A combination of therapeutic interventions did not yield any meaningful influences either (top half of Table 2).
The only meaningful treatment effect for subjective QoL was observed for a combination of treatments (g = 0.314, p = 0.036). None of the other examined interventions yielded summary effects that exceeded triviality or significance thresholds (excepting cognitive interventions, which yielded a significant, but trivial effect; bottom half of Table 2).
Regression analyses
In our meta-regressions, we investigated potential influences of eight predictors on effect sizes. Neither objective nor subjective QoL effects appeared to be significantly affected by any of the predictors, excepting for more positive influences of group therapy interventions for subjective QoL (Table 3). However, this significant result should be interpreted with caution because it may be a consequence of familywise error accumulation (i.e. Bonferroni-corrected significance levels for within QoL-domain regressions is 0.006 v. an observed p value for group-treatment of 0.021; see Table 3).
Table 3. Single precision-weighted multilevel regression models for objective and subjective QoL

a Referenced to inpatients.
b Referenced to individual treatment.
Summary estimates of treatment dependent symptom and functioning differences can be seen in online Supplementary Table S2 (positive signs indicate more beneficial effects of treatment compared to control groups). We used primary study effect sizes to predict subjective and objective QoL-related between-groups effects in a further set of single precision-weighted multilevel meta-regressions. In these analyses, positive effects of predictors can be interpreted as indicative for positive effects of treatments on the predictor side leading to positive effects on the outcome side (in other words, if treatments alleviate symptoms or enhance functioning, they also lead to more favorable QoL outcomes).
We observed significant positive effects of predictors for symptoms and functioning for objective QoL effect sizes, thus indicating more beneficial effects in treatment compared to control groups for both effect size types (top half of online Supplementary Table S3). Interestingly, predictor patterns were differentiated in regard to subjective QoL. Whilst functioning (barely) and total symptoms showed positive signs, positive, negative, and general symptoms predicted subjective QoL significantly negative (bottom half of online Supplementary Table S3). This may mean that treatment-dependent symptom changes are not linked to treatment-related favorable subjective QoL outcomes, but may even have adverse effects.
Dissemination bias
Visual inspection of contour-enhanced confetti funnel plots did not indicate funnel plot asymmetry of neither objective nor subjective QoL analyses (online Supplementary Figs 2 and 3, respectively). Our trim-and-fill analyses supported this interpretation, indicating no missing studies on the left-hand side of the summary effect estimate for either analysis.
Our three multilevel modeling-based approaches showed a consistent pattern of results within both analyses. Whilst no detection method indicated confounding influences of dissemination bias for objective QoL effects, all of them did so for subjective QoL.
On the one hand, for objective QoL neither Egger's regression test by means of sandwich estimators only, nor MLMA-based Egger's regression were indicative of bias (ps = 0.581 and 0.696, respectively). Furthermore, the three parameter selection approach showed no evidence for bias-related effect inflation (χ2(1) = 1.788; p = 0.181). On the other hand, for subjective QoL Egger's sandwich regression (p = 0.054), the MLMA-based Egger's regression (p = 0.024), as well as the selection approach (χ2(1) = 20.537; p < 0.001) yielded significant results, thus indicating an inflated summary effect.
Multiverse analysis
Specification curve
The descriptive specification curve indicated largely positive summary effects for objective QoL, with a median summary effect of g = 0.252 that ranged from g = −0.144 to 1.240 (25th and 75th percentiles indicated that 50% of values were between g = 0.055 and 0.415). All summary effects that reached nominal statistical significance had positive signs, thus indicating a rather robust beneficial therapeutic effect (Fig. 1). This may be interpreted as evidence for a robust, non-trivial, albeit small beneficial intervention effect on objective QoL compared to controls.

Figure 1. Descriptive meta-analytic specification curve of summary effects (Hedges g) for all reasonable specifications for objective QoL.
Note. The top panel shows summary effects with 95% confidence intervals in increasing order according to effect strength. This means that the leftmost effect represents the most negative effect that was observed according to any specification whilst the rightmost effect represents the most positive one. The y-axis provides effect strength in terms of Hedges g. The center panel indicates the number of samples within the data subset that a respective effect estimate is based on. The bottom panel indicates the combinations of specific characteristics in terms of selected data and which analytical approach was used to calculate the respective summary estimate. Warmer colors indicate lower precision (i.e. larger confidence intervals) of summary effect calculation. Confidence intervals that overlap with dashed reference line indicate non-significance of summary effect.
The largest positive intervention effects were observed when cognitive behavioral therapy or psychoeducation were used, although estimation precision was volatile. In terms of treatment type, our analyses showed that an exclusive use of group treatments yielded the least beneficial effects (or was even less favorable) compared to controls. For individual therapy and either therapy types, all summary effects were positive and predominantly significant.
For subjective QoL, effects were once again predominantly positive, albeit in general smaller and seemingly more likely to fail reaching nominal statistical significance. Effects ranged from g = −1.523 to 1.614 with a median summary effect of g = 0.137 (25th and 75th percentiles indicated that 50% of values were between g = −0.001 and 0.361). Most nominally significant summary effects had positive signs, although some specifications yielded negative signs (Fig. 2). These results show that evidence for a meaningful beneficial intervention effect on subjective QoL cannot be established. No clear pattern for drivers of influential moderator effects of factor levels was found, excepting an apparent tendency of lower treatment benefits when therapies were compared to other (non-therapeutic) control conditions.

Figure 2. Descriptive meta-analytic specification curve of summary effects (Hedges g) for all reasonable specifications for subjective QoL.
Note. The top panel shows summary effects with 95% confidence intervals in increasing order according to effect strength. This means that the leftmost effect represents the most negative effect that was observed according to any specification whilst the rightmost effect represents the most positive one. The y-axis provides effect strength in terms of Hedges g. The center panel indicates the number of samples within the data subset that a respective effect estimate is based on. The bottom panel indicates the combinations of specific characteristics in terms of selected data and which analytical approach was used to calculate the respective summary estimate. Warmer colors indicate lower precision (i.e. larger confidence intervals) of summary effect calculation. Confidence intervals that overlap with dashed reference line indicate non-significance of summary effect.
Combinatorial meta-analysis
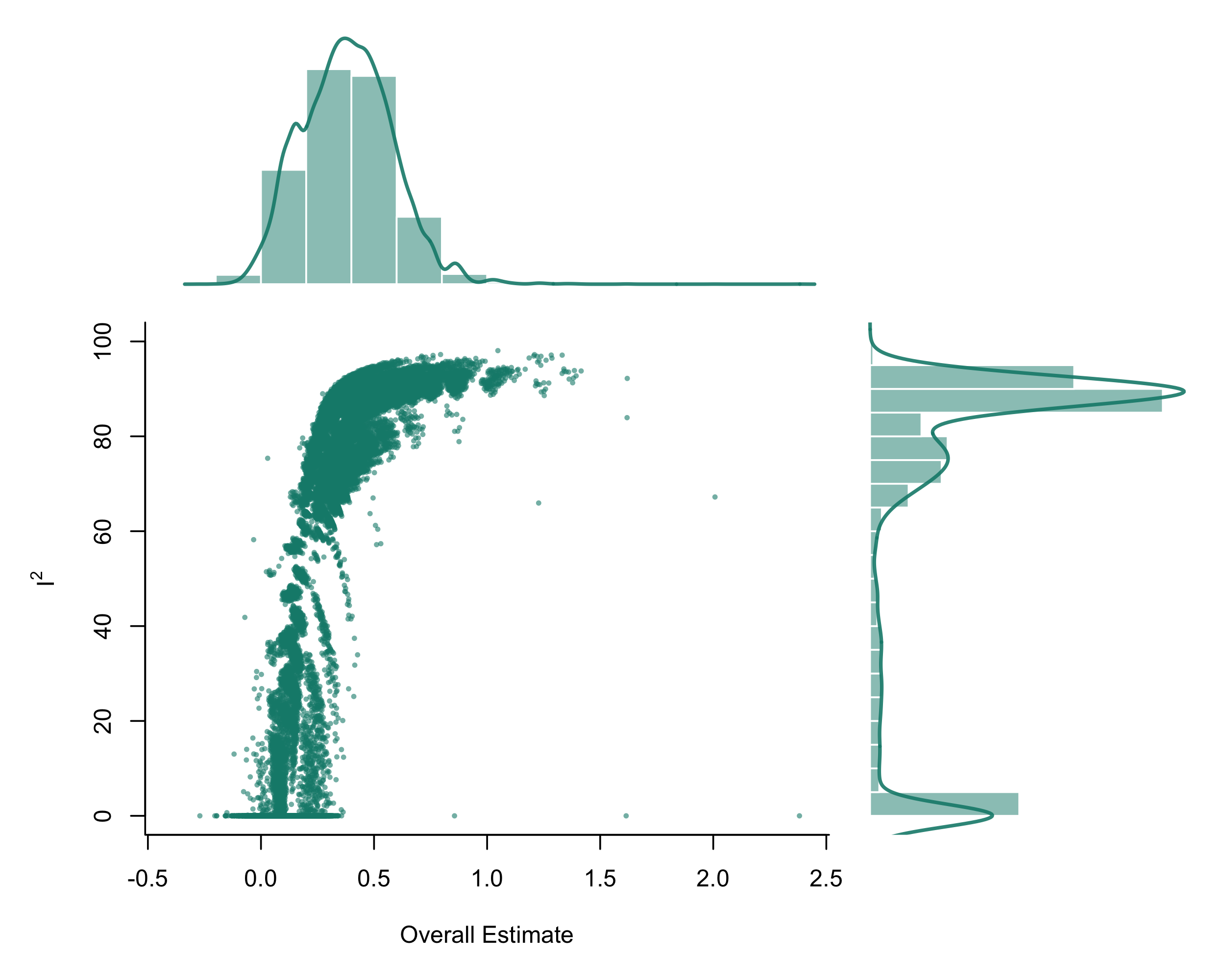
Random specifications of (unreasonable) combinations for objective QoL effects showed that summary effect estimations and between-studies heterogeneity seem to be systematically affected by the inclusion of certain studies (or study subsets). Visual inspection of GOSH-plots (online Supplementary Fig. S4) shows that larger effects are associated with larger between-studies variances. The median summary effect was somewhat larger than in specification curve analysis (g = 0.380; 25th and 75th percentiles = 0.239 and 0.513) with I 2 values indicating moderate-to-large between-studies heterogeneity (I-squared median = 85.03; 25th and 75th percentiles = 61.30 and 89.54) according to well-established heterogeneity thresholds (Higgins, Thompson, Deeks, & Altman, Reference Higgins, Thompson, Deeks and Altman2003).
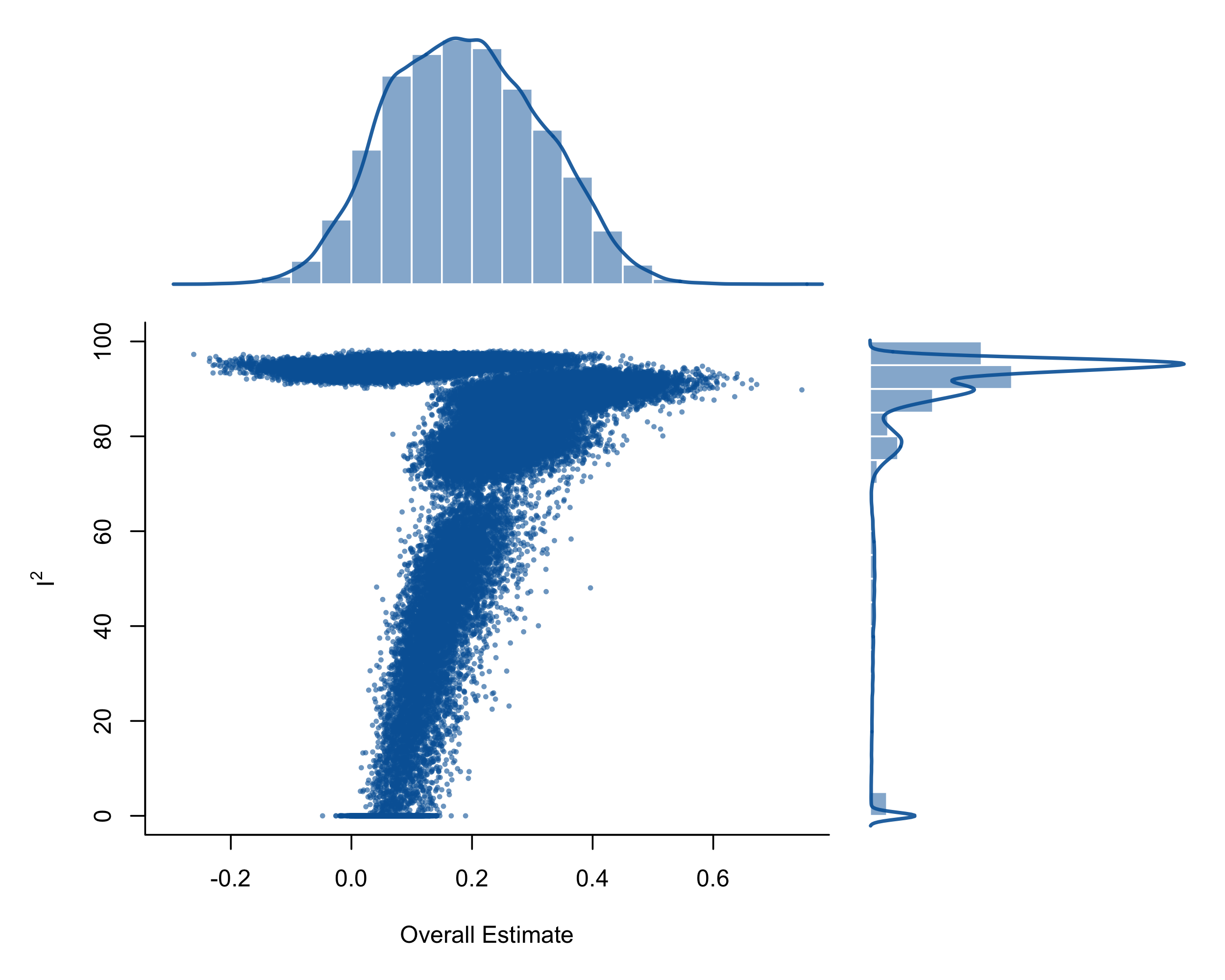
A similar pattern was observed for subjective QoL. Once again, the GOSH-plot revealed systematic associations of summary effect estimates with between-studies variability (online Supplementary Fig. S5), although largest variabilities appeared to be associated with lower effect sizes. The median summary effect was once more trivial (g = 0.185; 25th and 75th percentiles = 0.096 and 0.278) and I 2 vales indicated large between-studies heterogeneity (I 2 median = 92.48; 25th and 75th percentiles = 84.53 and 95.09).
In the light of these results, it cannot be ruled out that the presently observed pattern of effect size and between-studies heterogeneity differences for both objective as well as subjective QoL may be a consequence of unobserved systematic between-studies variance.
Discussion
Key findings
This meta-analysis aimed to contribute toward clarifying the effectiveness of different psychological interventions for improving QoL of patients with schizophrenia-spectrum disorders. The findings suggest that psychoeducation effectively improves objective QoL, and interventions that combine different therapeutic approaches (i.e. psychoeducation, CBT, problem solving, etc.) improve subjective QoL, although the effect is small. Group interventions seem to be more beneficial for improving subjective QoL, though this finding should be interpreted with caution. Importantly, the results suggest the existence of unobserved systematic between-studies variance for both subjective and objective QoL, thus indicating further systematic moderating influences that have not yet been identified. There were no indications for dissemination bias-related effect inflation for objective QoL, whilst some subjective QoL effects appeared to have been somewhat inflated.
Comparison with the existing literature
Our findings go beyond those of individual studies targeting QoL, providing a comprehensive systematic examination of therapy-dependent intervention effects. In this vein, our analytical approach allowed us a more fine-grained assessment of different intervention types and effectiveness on QoL compared to prior investigations (Correll et al., Reference Correll, Galling, Pawar, Krivko, Bonetto, Ruggeri and Kane2018; Laws, Darlington, Kondel, McKenna, & Jauhar, Reference Laws, Darlington, Kondel, McKenna and Jauhar2018; Valiente et al., Reference Valiente, Espinosa, Trucharte, Nieto and Martinez-Prado2019) as well as the first examination of their interactions. For instance, Laws et al. (Reference Laws, Darlington, Kondel, McKenna and Jauhar2018) examined the effectiveness of CBT on the recovery of patients with schizophrenia, including nine studies that targeted QoL as one of the outcomes, revealing no benefit for QoL. However, this conclusion may be misleading, because similar to Valiente et al. (Reference Valiente, Espinosa, Trucharte, Nieto and Martinez-Prado2019) (i) their meta-analytical results were based on studies including several different diagnoses (schizophrenia-spectrum and others) and (ii) no distinction was made in terms of objective and subjective QoL scores, thus leaving potential specific CBT-dependent therapy effects in terms of diagnosis or QoL type unclear. Our findings show that there is no meaningful effect of CBT on subjective QoL whilst the observed evidence for an effect on objective QoL remains ambiguous (i.e. despite an observed moderate effect, the associated confidence interval overlapped considerably with the null, thus leaving a potential advantage of CBT over TAU in need of substantiation), thus indicating that CBT does not improve QoL of patients with schizophrenia beyond treatment as usual. This is important, because CBT is the most widely used intervention for schizophrenia patients and recommended by the NICE guidelines as the gold standard (NICE, 2014).
Another prior meta-analysis (Correll et al., Reference Correll, Galling, Pawar, Krivko, Bonetto, Ruggeri and Kane2018) examined the effectiveness of Early Intervention Services (EIS) on several outcomes of patients with first episode psychosis. They included four studies about subjective QoL and revealed a weak effect. Given that EIS typically adopt a multidisciplinary approach involving psychological treatments but also occupational therapy, assertive management treatment, carer support, etc., it is not possible in such primary studies (and resulting meta-analyses) to untangle effects of specific psychological treatments, which limits the validity of their reported treatment effects.
It is worth noting that the majority of the included studies focus on subjective QoL, whilst objective QoL is less often targeted by psychological interventions. This may be explained by the priority in inclusion of (subjective) QoL as a patient reported outcome, instead of its inclusion as an observer-rated outcome. However, our results of overall intervention effectiveness on objective QoL indicate that this outcome is very relevant as a criterion for testing interventions, though it has been suggested to more closely represent indicators related to standards of living, or ‘quality of living’, rather than QoL (Awad & Voruganti, Reference Awad and Voruganti2012).
Our moderator analyses suggest that symptom-alleviating and functioning-improving interventions substantially ameliorate objective QoL. This idea is consistent with the well-established negative relationship of objective QoL with symptom severity (Eack & Newhill, Reference Eack and Newhill2007). This means that an overall improvement of the clinical condition can be expected to improve a given patient's life conditions. These findings are consistent with the previously observed strong relationship of overall functioning with objective QoL (Nevarez-Flores et al., Reference Nevarez-Flores, Sanderson, Breslin, Carr, Morgan and Neil2019). Of note, our results indicate that when positive, negative, and general symptoms improve, treatment group patients provide more negative evaluations of their life conditions than control group patients. This may be explained by the ‘insight paradox’ (Davis, Lysaker, Salyers, & Minor, Reference Davis, Lysaker, Salyers and Minor2020). That is, patients with increased disease awareness perceive their (subjective) QoL worse than those with poor insight. This phenomenon is exacerbated for people with decreased symptomatology. As the person gets better, they begin to have a better understanding of how their life is constrained by psychosis, and thus appraise their life conditions in a more negative way.
Moreover, our findings show that group interventions are more effective in improving subjective QoL compared to individual or combined format interventions. These findings are in line with prior evidence on social functioning (Orfanos, Banks, & Priebe, Reference Orfanos, Banks and Priebe2015) and may reflect well-established beneficial effects of group therapy for patients with psychosis (Kanas, Reference Kanas1996). Typically, this increased effectiveness is attributed to groups offering such patients an opportunity for experience sharing and relationship establishment with people that share similar concerns toward life. However, this finding should be interpreted with caution because the nominal statistical superiority of group interventions disappeared when correcting for statistical family-wise error accumulation.
Strengths and limitations
Our present approach allowed us to provide the first meta-analytical evidence of specific intervention effects on QoL in patients with schizophrenia-spectrum disorders based on the so far most comprehensive data and analyses of this topic. Specifically, we were able to (i) disentangle differential treatment effects according to specific QoL outcomes, (ii) assess influences of different intervention types, (iii) examine moderating effects of sample-level characteristics as well as their interactions within moderators and design variables, (iv) investigate evidence for effect inflation due to dissemination bias, as well as (v) explore the impact of researcher degrees of freedom-dependent (un-)reasonable decisions in terms of data selection and ways to analyze them in multiverse analyses.
However, some limitations should be noted. First, we did not distinguish between self-reports of subjective and health-related QoL in our main analyses, thus potentially introducing statistical noise. However, supplementary separate analyses for both health-related and subjective QoL yielded virtually identical results (omitted for brevity). Second, we included studies assessing QoL based on the EQ-5D questionnaire, which in the past raised concerns regarding the extraction of conclusions on the individual QoL rates of patients with psychosis (Brazier, Reference Brazier2010). However, more recent evidence suggests that this instrument provides reliable QoL assessments to be used for group comparisons (Barton et al., Reference Barton, Hodgekins, Mugford, Jones, Croudace and Fowler2009; Pitkänen et al., Reference Pitkänen, Välimäki, Endicott, Katajisto, Luukkaala, Koivunen and Hätönen2012). Therefore, we considered studies using EQ-5D to be eligible for answering our research question. Third, WHO-QoL subscale scores were averaged for our multiverse calculations. This was necessary to allow an examination of the impact of moderator interaction effects because multilevel modeling is currently unfeasible in this approach. Fourth although it is highly recommended to use disease-specific instruments when the aim is to detect treatment effects (Karow, Wittmann, Schöttle, Schäfer, & Lambert, Reference Karow, Wittmann, Schöttle, Schäfer and Lambert2014) this was only observed for objective QoL (i.e. using the QLS) whereas most studies targeting subjective QoL used a variety of generic assessments (i.e. not specifically designed for assessing QoL in patients with schizophrenia, such as the WHO-QoL; MANSA, Q-LES, etc.). Also, although all QoL instruments employed in the included studies have been widely used within this population, none of the instruments follow the Patient-Reported Outcomes Measurement Information System (PROMIS) (Cella et al., Reference Cella, Riley, Stone, Rothrock, Reeve and Yount2010), which would allow for more accurate comparisons across studies. Fifth, only few studies reported outcomes of intention-to-treat analyses. Therefore, a completer-only bias may have contaminated our findings. Given the small number of studies that followed this approach, it was not possible to test for this bias using sensitivity analyses. This limitation illustrates that gold standard approaches of RCT-based reporting (see for instance CONSORT checklist item 16; Schulz, Altman, & Moher, Reference Schulz, Altman and Moher2010) is still insufficiently practiced. Sixth, the results of the presently meta-analytically summarized data should not be generalized beyond the context of Western countries, due to the majority of included studies having been conducted in WEIRD (Western, Educated, Industrialized, Rich, Democratic; Henrich, Heine, & Norenzayan, Reference Henrich, Heine and Norenzayan2010) countries.
Implications for research and practice
In all, our findings suggest that the interventions' benefits vary based on outcome and intervention type. We purposefully excluded studies that included patients with diagnoses other than schizophrenia (i.e. bipolar disorder, depression). Though one may argue that interventions offered in the context of mental health services should adopt a transdiagnostic approach, focusing on the patients' reported difficulties instead of their symptoms, it has often been shown that QoL differs among diagnostic populations (Ådnanes et al., Reference Ådnanes, Kalseth, Ose, Ruud, Rugkåsa and Puntis2019; Berghöfer et al., Reference Berghöfer, Martin, Hense, Weinmann and Roll2020; Petkari & Priebe, Reference Petkari and Priebe2023) and this may impact the intervention effectiveness. Therefore, future studies should either target populations with refined diagnostic criteria, or at least compare the outcomes of different diagnostic subgroups receiving the same intervention. Even within the schizophrenia spectrum, our findings revealed a trend of diagnosis as moderator of the intervention effectiveness. That is, interventions may be more effective when targeting samples of schizophrenia patients only, compared to when targeting patients within the whole schizophrenia spectrum (schizoaffective, delusional, etc.). Therefore, to be able to extract refined conclusions about what works for whom, future studies need to provide more information on how interventions benefit patients with different diagnoses within diagnostic subgroups.
Also, although illness duration did not emerge as a meaningful moderator, QoL levels and determinants may differ between patients with early psychosis and chronic patients (Gardsjord et al., Reference Gardsjord, Romm, Friis, Barder, Evensen, Haahr and Røssberg2016). In our analysis, there were only four studies focusing on samples with early psychosis, two targeting objective QoL and two subjective QoL, therefore a comparison with more chronic samples was not possible. Given the importance of the first-five-years-from-onset period for determining functional outcomes (Crumlish et al., Reference Crumlish, Whitty, Clarke, Browne, Kamali, Gervin and O'Callaghan2009), further RCTs that target QoL are needed to determine the best intervention to implement with these patients.
Moving beyond this in this meta-analysis we did not test the intervention effects on different QoL dimensions (i.e. environment, health, living conditions), as QoL scores were considered as a whole. The scores on QoL dimensions may be fluctuating (Berghöfer et al., Reference Berghöfer, Martin, Hense, Weinmann and Roll2020), with patients for instance reporting high appraisal of environment, but not of social relationships; therefore, there may be a differential effect of interventions depending on the QoL dimension under study. Future studies are encouraged to report scores on QoL dimensions to be able to detect potential intervention targets.
Furthermore, interventions based on a variety of different approaches (i.e. systemic, psychodynamic art-therapy, mindfulness, etc.) were considered together under the umbrella of ‘other’, because there were not enough studies for creating dedicated categories. Future studies are needed to disentangle their effects based on robust RCTs. For instance, third generation approaches seem to be promising for improving QoL, but the evidence is still scarce (Jansen, Gleeson, Bendall, Rice, & Alvarez-Jimenez, Reference Jansen, Gleeson, Bendall, Rice and Alvarez-Jimenez2020).
According to our results, psychoeducation improves objective QoL, suggesting that receiving information on how to handle the disorder and its consequences may help the person to ameliorate their life conditions; however, this finding should be interpreted with caution, because it is based on two studies only. Combined interventions seem to work better for improving subjective QoL. Given the variability among the included multicomponent interventions, extracting results on what exactly works is quite challenging. What these interventions have in common though is that they are all manualized and multifaceted, targeting a series of elements within the same program, such as education on the disorder characteristics, problem solving, emotional and cognitive skills. Therefore, they may be an ideal candidate for improving the patient's life appraisal.
Conclusions
The findings suggest that QoL is a valid outcome criterion for assessing psychological interventions, as it is sensitive to change. However, the effect is small and there is large variability depending on the QoL and intervention type, which call for the testing of new solutions. This testing should be conceived either in terms of more in-depth examinations of different intervention types (i.e. included in this meta-analysis under the umbrella of ‘combined’ and ‘other’) that may ameliorate QoL, or in terms of focusing on different QoL dimensions that may be more plausible to target through the available interventions.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291723003070.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interest
The authors declare none.