
In the Introduction we detailed how our lived experiences – as Black women, as therapy clients, as clinical mental health practitioners and educators, and as workshop leaders advocating for multicultural competence in the mental health profession – have vastly enriched our approach to this book. We have counseled Black women of different ages and stages in life spanning more than two decades. We have also mentored, educated, and trained others seeking to become mental health practitioners. The rationale, assumptions, and themes that guide our work have been shaped by the views of hundreds of Black women we have encountered in our work. Yet we want more. We want to include the voices and direct feedback of Black women, who should play a vital role in determining the nature and quality of mental health services they receive. To accomplish this goal in the book, we collated Black women’s viewpoints and recommendations via a research study, that was completed before we wrote one line of this text.
In this chapter we provide a brief summary of the study goals and methods with a more detailed write-up in the Appendix. We also provide a detailed overview of the main study with other results integrated into specific chapters.
1.1 Study Aims
The Black Women and Psychotherapy study was an exploratory and cross-sectional examination of Black women’s thoughts and opinions on professional therapy services. The study aims were (a) to understand Black women’s perspectives on professional psychotherapy services, (b) to understand Black women’s experiences in professional psychotherapy services, and (c) to collate Black women’s recommendations for mental health practitioners who work with Black female clients. We gathered Black women’s opinions to validate the topics and strategies we recommend in this publication. We also wanted to offer therapists some concrete, empirically informed recommendations on working with Black female clients. We conducted the study in the traditions of survey research using quantitative procedures and descriptive statistics to summarize overall participant ideas. We also used qualitative procedures and techniques to elicit and report Black women’s recommendations for therapists. Northwestern University’s Institutional Review Board approved the research. See the Appendix for more details on the research framework.
1.2 The Sample
We targeted a sample of 100 Black women across a geographic and demographic spectrum. We were pleasantly surprised to have 100 participants complete the surveys within a week of launching; however, early data showed a lack of diversity on critical demographics (e.g., age, education, income, US region). We wanted a highly diverse sample, so we conducted further outreach in communities such as churches, local social agencies, and sororities to attract more Black women from the South and those of lower education and income levels. We also asked colleagues residing in the South and working with low-income Black women to distribute our recruitment details to their networks. The final sample of 227 Black women who completed the survey were more diverse, yet there was still limited participation of one demographic of interest, low-income Black women, with less formal education. See Appendix for inclusion criteria, recruitment, and informed consent procedures.
1.3 The Survey
We distributed the anonymous Qualtrics survey to Black women who had never been clients in therapy as well as those in therapy currently or in the past. The survey included five sections: (a) an introduction to the study; (b) informed consent information; (c) personal and demographic questions; (d) questions about therapy among both clients and those who were never clients; and (d) four open-ended questions asking about the helpfulness and unhelpfulness of therapy, why Black women avoid therapy, and Black women’s recommendations for therapists working with Black female clients. The final survey ran from July to September 2020. The survey is available on request from the authors. See the Appendix for how the Qualtrics survey was developed and presented and for data analytic strategies.
1.4 Study Findings
1.4.1 Participant Characteristics
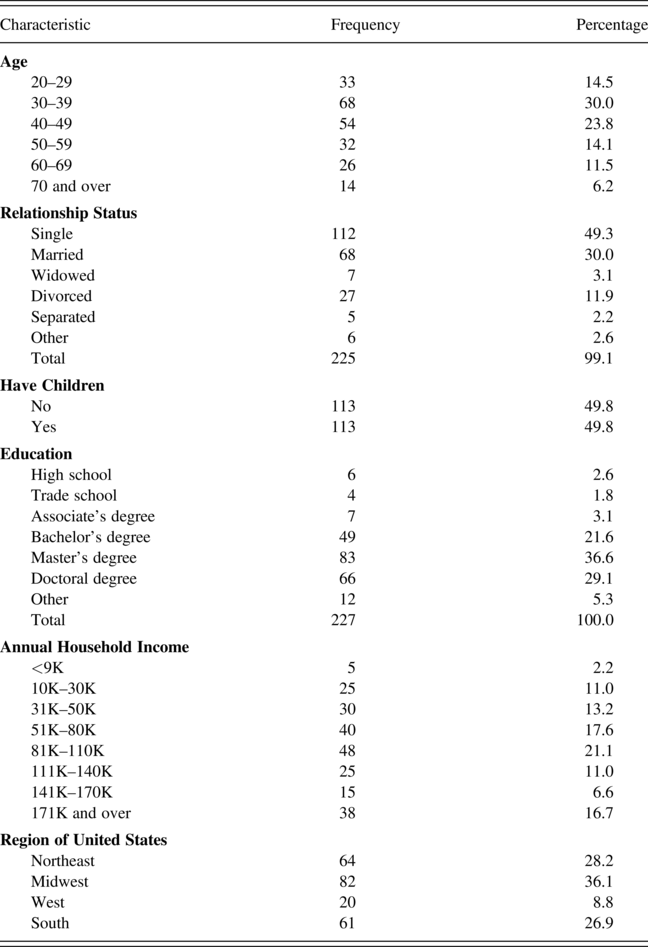
A total of 293 individuals began the study, 227 of them met our criteria, and we analyzed their data. Sixty-six individuals completed the requirements to be included and started the research but ended early, and we did not analyze their data. Table 1.1 lists the demographics of the 227 participants remaining in the sample. Most participants (96%) identified as Black. Eight individuals identified as multiracial (including Black). Among the participants, 99% identified as female, with one individual identifying as nonbinary, and 96% identified as non-Hispanic Latino.
Table 1.1 Sample characteristics
We were pleased to get a sample of predominantly Black women from all over the United States who met our study criteria. Black women from the South, Midwest, and Northwest were well represented; the western part of the United States was less well represented. There was nothing remarkable about the sample’s age distribution, marital and partner status, the fact that half had children, and the fact that most (69%) reported being very religious/spiritual. One limitation is the lack of diversity in income and education of the Black women in the study. The Black women in our sample are primarily well-educated, cisgender women with relatively high household incomes. Most of our participants (85%) were college educated with at least a bachelor’s degree, and more than 50% had graduate degrees. Less than 10% reported an associate degree or less formal education. Roughly 55% of the sample had annual household incomes of $81,000 and above. We value the perspectives of well-educated Black women with above-average household incomes. However, we also really wanted to include Black women who had less education and fewer financial resources. We were disappointed to have so few in the sample, as we had hoped to better understand the opinions and experiences of a less privileged group of women, such as those with less formal education and household income.
Nevertheless, the fact that Black women who had therapy were overrepresented in our sample has significant benefits. The overrepresentation of Black women who have been in therapy provides us with responses based on real, lived experiences of therapy. These data proved to be immensely useful. A more representative sample may have given important opinions on a number of prospective therapy benefits, yet offered us fewer insights into the lived experiences of clients in therapy because many participants would not have had real-life experiences on which to draw.
1.4.2 Views on Finding and Using Therapy
A substantive majority of respondents (N = 192, 84.6%) had therapy, a much smaller number (N = 28, 12%) had never thought of having therapy, and even fewer (N = 7, 3%) tried to get therapy and then changed their minds. Of the 192 who had therapy, 70% were clients for three years or less. As for the number of therapists, 61% worked with one or two therapists, and around 8% had worked with three or more. Responses on the ease of finding a therapist were mixed: 41% found it difficult or very difficult to find a therapist, while 41% found it easy to very easy. In terms of how participants found their therapists, sources were personal referrals (49%), an internet site (30%), insurance (28%), a physician’s recommendation (13%), a job referral (10%), an advertisement (5%), or a business card (1%).
Around 85% of our sample had professional therapy, which was likely associated with their income and educational status. Most of the participants were college educated, and more than half had graduate degrees. More than half also had annual household incomes of $81,000 or more. These Black women also likely had stable jobs. The findings in these dynamics did not surprise us. Black women who are well educated and have high income are also more likely than people with low income to have insurance coverage around which they can seek mental health services.
1.4.3 Therapist Preferences
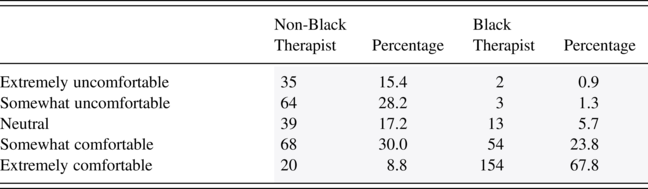
Of those who had been in therapy, we asked, “What did you look for in a therapist?” Table 1.2 includes all qualities endorsed. The top five preferences were therapists who had experience with people of color (67%), took insurance (59%), have cultural knowledge (55%), had the educational background (master’s degree or PhD) and professional license to practice (51%), and were of the same sex or gender as the respondent (50%). The least preferred qualities were spiritual or religious emphases (26%) and therapist age (18%).
We asked participants to indicate their comfort level working with both Black and non-Black therapists (Table 1.2). Among our sample, 38% would be comfortable or extremely comfortable working with a non-Black therapist, 17% would be neutral, and 44% would be somewhat uncomfortable to very uncomfortable working with a non-Black therapist. Alternatively, 91% of our sample of Black women would feel comfortable with a Black therapist.
The predominance of finding a therapist through a personal referral aligns with our experience in practice. Our Black clients and other people of color who seek our services tell us that they have looked long and hard to find a Black therapist. About 41% of our sample found it difficult or very difficult to find a therapist. It may be that Black women are waiting to find a Black therapist, and there are pros and cons to this strategy. The likelihood of finding a Black therapist is low because there are relatively few in the field, less than 5% nationally (Hamp et al., Reference Hamp, Stamm, Lin and Christidis2016; Lin et al., Reference Lin, Stamm and Christidis2018). Waiting to find a Black therapist means that women may struggle with mental and emotional health conditions for quite a while without being seen. This idea underscores our invitation to Black women in various chapters of the book, to expand their therapy options to consider non-Black therapists. The limited availability of Black therapists to work with Black women also increases our interest in supporting non-Black therapists to work competently with this population.
Notably, while Black women might look first for a Black therapist, more than half would be neutral to very comfortable working with a non-Black therapist. Personal referrals can go both ways. People will refer a therapist of any race or ethnicity with whom they have had good experiences and whom they trust. The rise of internet-based sources for seeking therapy should increase therapists’ interest in listing their business on sites like Therapy for Black Girls or Psychology Today. We recommend that therapists of any background design a culturally attuned profile on internet sites that signals their cultural proficiency and interest in working with people of color. In these profiles therapists should also indicate themes that may resonate with Black women.
1.4.4 Life Satisfaction and Mental and Emotional State
We asked two questions to assess our participants’ subjective sense of navigating life, given that we collected data during the COVID-19 pandemic and quarantine. The first question was “How satisfied are you with your life overall?” In response, 72% reported being somewhat to extremely satisfied. This finding confirms other studies that, in general, Black women are apt to feel satisfied with their lives despite the difficulties they may experience (Winfrey-Harris, Reference Winfrey-Harris2015). Another question was “What is your current mental and emotional state?” Over 70% of Black women in the sample described their mental and emotional state as neutral to poor. A Pearson chi-square test showed a statistically significant relationship between annual household income and current mental and emotional state. A little over half (53%) of participants who reported a good mental and emotional state had higher household incomes of $81,000–$110,000 (28%), closely followed by those with incomes of $51,000–$80,000 (25%). There is a positive connection between mental and emotional status and economic status. Still, we view these findings with some caution given the small number of low-income women in our sample.
The finding of neutral to poor mental and emotional state among most of our study sample of Black women is disheartening but not surprising. Indeed, COVID-19 and quarantine conditions have taken a toll on people’s mental and emotional health worldwide, and many people, including Black women, are feeling these effects. A pandemic of mental health vulnerability is quietly unfolding alongside the virus, occurring on the racial and ethnic spectrum. People of color seem to be uniquely affected in significant ways. Compounded with COVID-19 conditions, Black people are experiencing the mental health impacts of police killings of Black people, the mass riots around antiracism, and the rise in White nationalism (Floyd, Reference Floyd2020; Gaines, Reference Gaines2020). Media reports indicate that Black therapists see a dramatic increase in help-seeking from Black people (Gaines, Reference Gaines2021). We expect this trend to continue for some time. Black women are in desperate need of therapy. We believe they would be willing to try any therapist who welcomes them and shows interest in working with them through the contexts of their lives.
Chapters 6 and 7 discuss how therapists can be ready to showcase familiarity with people of color and cultural knowledge to build alliances and a welcoming environment for Black women.
1.4.5 Reasons for Feeling Stressed
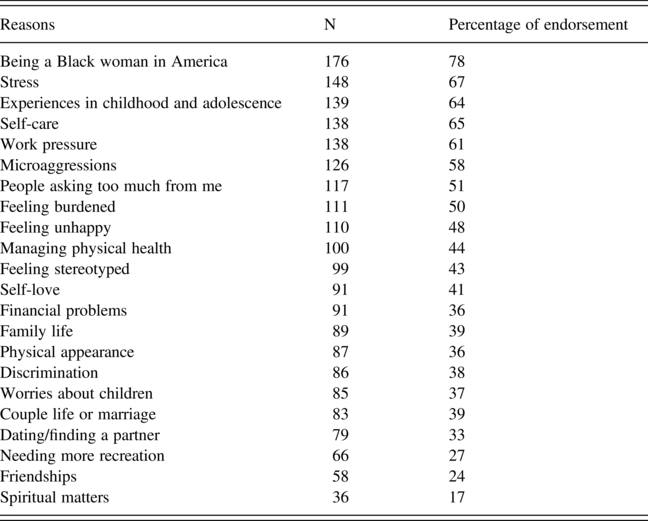
We asked participants why Black women might feel distressed. Women were allowed to endorse any of the listed conditions that applied. Table 1.3 lists the endorsements of multiple conditions. The top conditions endorsed by participants were being a Black woman in America (78%), experiencing stress (65%), childhood and adolescent experiences (61%), work pressure (61%), and self-care (61%). Notably, almost all stressors from the list provided to participants were endorsed.
Table 1.3 Reasons Black women might feel distressed
1.4.6 Reasons for Seeking Therapy
Table 1.4 lists participants’ endorsement of reasons they sought therapy among all that apply. The top reasons were stress (64%), a mental health symptom such as depression (63%), self-care (48%), couple or dating problems (38%), or family issues (34%). The least endorsed reasons were spiritual and religious concerns (7%).
Table 1.4 Reasons Black women seek therapy
The top list of stressors affecting Black women in the study and the top reasons for seeking therapy match our experiences in practice. Black women are apt to begin therapy with relatively straightforward narratives, but right below their initial story lines are other layers of information related to the stressful conditions of their lives based on gendered racial dynamics. This is captured in the sentiment that some of their difficulties relate to being a Black woman in America. Among several endorsed circumstances and stressors are those this book addresses. Several chapters touch on the primary stressor, which is being a Black woman in America. This stressor relates to women’s experience of gendered racism and other oppressions based on their social identities. Along with these experiences come microaggressions and experiences of discrimination in multiple contexts. Women’s family contexts are also among the reasons for stress or therapy seeking. They include coupling or dating, family life, parenting, or caregiving. Black women’s girlhood or childhood and adolescent experiences are also endorsed.
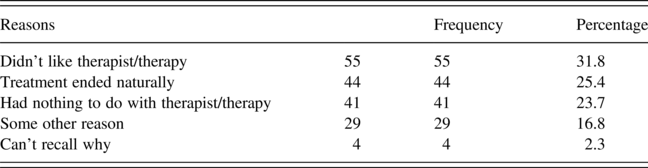
Table 1.5 Reasons for ending therapy
| Reasons | Frequency | Percentage | |
|---|---|---|---|
| Didn’t like therapist/therapy | 55 | 55 | 31.8 |
| Treatment ended naturally | 44 | 44 | 25.4 |
| Had nothing to do with therapist/therapy | 41 | 41 | 23.7 |
| Some other reason | 29 | 29 | 16.8 |
| Can’t recall why | 4 | 4 | 2.3 |
1.4.7 Reasons for Ending Therapy
We asked participants why they ended therapy. Around 32% terminated because they did not like their therapists. We found these results surprising and encouraging because in our experience, when clients do not feel that therapy or a therapist is helpful, they drop out. Our data suggest that nearly two thirds of clients in our sample terminated therapy for reasons that had nothing to do with the therapists or the therapy ended naturally or for other reasons.
1.5 Qualitative Findings in Open-Ended Questions
1.5.1 What Questions Were Asked
Our survey included four open-ended questions. All participants were asked two questions: “Why might some Black women avoid therapy?” and “What are your recommendations for therapists who work with Black women as clients?” Two questions went only to those who had therapy: “Overall in therapy, what has been helpful to you?” and “Overall, in therapy, what has not been helpful to you?” We were pleased to receive 792 unique statements in response to the four questions, with participants writing several lines of text. We consider this one of the richest data sources in our study.
To analyze themes in Black women’s statements, we worked with a qualitative data Reference BrendalyconsultantFootnote 1 and three research assistants (RAs) to assist with coding and thematic analyses of these data. Our RA coders were 3 graduate students in their 20s studying to be mental health practitioners. The three RAs identify as Black, Black and biracial, and White, and all three identify as women. We followed strategies recommended by Braun and Clarke (Reference Braun, Clarke, Cooper, Camic, Long, Panter, Rindskopf and Sher2012) to discern commonalities, nuances, and meanings in participant comments. Our goal was to elicit specific and overarching themes in Black women’s perspectives. Coding procedures are detailed in the Appendix.
Following our RAs’ initial coding of responses, we reviewed the coding, examined themes across the 792 unique statements, and identified core themes, subthemes, and interconnections among the themes. This process exposed the subtleties in participant views that revealed how the meaning of some of participants’ sentiments shifted depending on the context. For example, the theme of time was a barrier to seeking therapy and related to lack of time to visit a therapist because of various responsibilities. However, under the question of recommendations for therapists, time was related to wanting longer sessions with the therapist to discuss serious issues. Next, we asked questions of the data: How do the women talk about their experiences related to the four questions? What assumptions do women make in the interpretation? What kind of worldviews emerged through their narrative account? Following this thematic analysis, we evaluated all statements for meta-themes present among all four questions. In the following discussion, all italicized words are verbatim from our study participants.
1.5.2 Views on Why Some Black Women Avoid Therapy
We analyzed 220 unique statements from participants and found two core themes related to Black women’s avoidance of therapy. The first was that Black women might avoid therapy out of fear of violating sociocultural norms. Subthemes were that Black women might fear stigma, might violate a strong Black woman image or family trust, and might violate their religious faith or values. For example, one participant noted reasons that Black women might avoid therapy:
Because of the stigma of therapy. Often, and especially for Black women who grew up as Christians, we’re told that we just need to pray our struggles away, that a deepening of faith will reduce our troubles; so, it can be hard to reach out when the people (usually women) around you characterize all issues as a result of a lack of sufficient faith.
Overwhelmingly, Black women used the term stigma to express this fear of violating norms in the larger society, the Black community, and the church. Women’s fears seemed connected to being a Black female. Fears also seem related to being perceived as crazy, weak, lacking in faith, and not handling business or keeping business private. Women described not wanting to be stereotyped, judged, ridiculed, shamed, or in a position that would negatively impact their employment or in child custody matters.
The second core theme of why Black women might avoid therapy was lack of access to some resources. Subthemes around a lack of access to resources were finances or cost, time, information, and how to find a good therapist. Finances or cost was the most referenced factor. Women noted the cost of therapy in general and connected cost to lack of insurance or limited insurance and high out-of-pocket expenses:
Therapy has a notorious reputation for being expensive and I don’t know that the profession does a good job at explaining how therapy can be made affordable for financially strapped people.
The second most referenced subtheme related to a lack of access to resources was lack of time. This was expressed as a lack of time to attend therapy due to professional and family responsibilities. The subtheme of finding a good therapist seemed to relate to the daunting task of finding a therapist to trust. For participants, it appeared that they lack knowledge of how to find the right therapist.
Though I spend most of my time in the Midwest, I’m originally from the South, where it can be difficult to find therapists (especially Black women) outside of a handful of major southern cities.
Women in the study referenced connecting or identifying with someone. Therapists that understand their experiences and culture seemed to be viewed as the right match.
Not finding a therapist they can identify with. Feeling weak. Having time and other resources to direct to self-care. Unable to focus on therapy because of other overwhelming day to day issues with surviving in America as a woman of color.
Some participants noted the difficulty of integrating therapy into their everyday lives:
Because having to open boxes that you have had to emotionally lock to survive can be difficult… . Who puts you back together when you are all alone in the evening after you have [bared] your soul that afternoon.
Other participants talked about how the idea of seeking therapy seemed to contradict how they had been raised:
I think some black women avoid therapy because we feel like we don’t need it. Black women are raised to be strong, fierce, brave, and solid. We are taught to fight through whatever we go through alone. That is what we have always seen.
1.5.3 Views on What Has Been Unhelpful in Therapy
We identified several core themes in Black women’s comments about what was unhelpful in therapy. Core themes were lack of cultural competency in therapists, consequences, unsupportive interactions in therapy, challenges in the process, lack of rapport, lack of structure, unprofessionalism, time, and cost. Lack of cultural competencies was in the context of therapists not having the same cultural background as participants. This seemed to make Black women perceive that therapists might be unfamiliar with the issues and experiences of Black people in the United States. One participant stated:
My current counselor is a White woman and she doesn’t broach topics of race or discrimination … she will talk about it if I bring it up but she won’t introduce it and we don’t really go into a lot of depth about it.
Black women participants commented on the therapist’s unwillingness to go in depth on cultural issues and the inability to navigate or integrate a religious perspective. Other contexts were having to teach therapists on topics such as intergenerational trauma. Examples of the consequences of unhelpful therapy were making clients feel minimized or dismissed.
Lack of supportive interactions included the therapist not listening, talking too much, or focusing on matters unrelated to the client’s goals. Other examples included the therapist having a posture as though listening to gossip and being focused on diagnosis instead of listening. The challenges in the process on the client’s side were difficulty being open or vulnerable, talking about painful things, and baring your soul.
It can force you to confront things all at once sometimes, and that can be overwhelming. You can get the sense that maybe you need to address big questions or “issues” about yourself right now when without therapy, you would have continued being *fine*, or just dealt with those issues in your own time. Overall this is probably a positive thing but it can cause stress in the moment. Additionally, sometimes it can feel like every little thing about how you think needs to be explored or broken down and sometimes, you just don’t want to bother – you sometimes can have a natural inclination to leave certain things as is but when in therapy, you can mention something in passing that you don’t feel like exploring but then you sometimes have to, and that can be difficult or frustrating. Similar to my last point, however, I assume that these types of discomfort are overall positive in the long run.
Related to therapist’s qualities, dislikes included unhelpful interventions such as homework.
Sometimes it can feel like every little thing about how you think needs to be explored or broken down and sometimes, you just don’t want to bother – you sometimes can have a natural inclination to leave certain things as is but when in therapy, you can mention something in passing that you don’t feel like exploring but then you sometimes have to, and that can be difficult or frustrating. Similar to my last point, however, I assume that these types of discomfort are overall positive in the long run.
The therapist’s emphasis on matters that are not helpful to Black women was also mentioned.
In the past I had a counselor who was a Black woman but I didn’t think she was attentive enough and she was a bit pushy – kind of telling me what she thought I needed and how the session would go … none of that was helpful for me.
Challenges in the process related to how much time must pass to go deep and feelings of insecurity. Lack of professionalism included therapists falling asleep. Other respondents felt the therapist was overworked and needed money. Other examples were therapists talking about their own problems, rescheduling, being late, or engaging in distracting behaviors like chewing gum or playing with her hair. Another mention was the therapist seeming in awe of clients’ lives versus providing help.
In the question of unhelpfulness of therapy, comments about time related to participants feeling rushed through the process, the time it takes to open up to the therapist, the number of sessions, the therapist’s inflexibility regarding scheduling, the search process to find a therapist, and feeling like therapy was unproductive or a waste of time. The context of cost seems to relate to therapy being way too expensive, therapy not being successfully covered by insurance, or the therapist not taking my insurance. Costs and time of therapy are discussed later in this chapter as one of the meta-themes cutting across numerous responses.
1.5.4 Views on What Has Been Helpful in Therapy
The first core theme in the helpfulness of therapy was related to having a safe space. Subthemes were being able to express feelings, confidentiality, being honest, a space for healing, a trusting environment, and a space to vent without opinions or reactions. Participants appreciated:
Having a therapist who listens, validates my experiences, nonjudgmental, and also helps me discover insight and practical ways of dealing with issues.
They also appreciated:
Developing a sense of self-worth, because I was given a safe space to share my concerns, doubts, and uncertainty. In that space my concerns were validated, and that validation allowed me to begin recognizing my needs. Once I recognized my needs, I was able to begin communicating them and doing things that affirmed my worthiness.
A second core theme in the helpfulness of therapy was positive outcomes with subthemes of tangible benefits such as healing, coping, insight, guidance on managing mental health, and self-care. This sentiment unfolded in the context of actionable advice, self-care strategies, and improved quality of life.
As someone who doesn’t generally share thoughts and feelings with anyone, I’ve appreciated having a safe, confidential space in which to just say things out loud without having to censor myself. I’ve also learned some really great ways to help manage some of my mental health issues, which has made life much less of a struggle. I also appreciate having a different perspective on happenings in my life.
The third core theme in therapy helpfulness was that the therapist had cultural and gender competence. Contexts were knowing African American culture and having a therapist who looked like us. This theme also seemed related to incorporating spirituality and feeling that therapists understood Black women.
1.5.5 What Are Recommendations for Therapists Who Work with Black Women?
Recommendations for therapists include two core themes. The first was cultural competency. Cultural competency subthemes that emerged are learning about Black women or Black people, researching, asking questions, being aware of bias, and speaking honestly. Cultural competency seemed strongly connected to Black women’s comfort in sessions and perception of the therapist’s ability to help them. Learning about Black women’s dual identities (race and gender) and experiences in the United States and their culture were the contexts in which sentiments appeared. Some women do not want to “explain culture” to the therapist.
One of the reasons I sought the therapist that I have is because I knew that there was a good chance that I would not have explain some of my experiences, both personal and professional, because there would likely be commonalities due to my therapist’s demographics. Where those commonalities don’t exist, I think it’s incumbent upon the therapist to do the extra work to ensure that they understand the unique burdens we face.
Another participant echoed the need for cultural understanding:
If a therapist is working with Black women, they really need a deep understanding of the double burdens that come with being both Black and a woman in a nation that is notoriously hostile to both of those demographics. For non-Black and non-women therapists, I think this understanding has to come from extensive, and regular, self-education.
The second core theme among recommendations related to fostering supportive interactions in therapy. Subthemes were listening, affirming, patience, empathy, not judging, building rapport, trust, and treating me as an individual. Supportive interactions focus on how Black women wanted to be treated. The most referenced subtheme carried the connotation of listening. Listening appeared in the context of being heard and in several individual statements. Regarding recommendations for therapists, listening was important in the context of the larger society and their communities. Black women express not always being heard.
I think all therapists should really be careful about diminishing the perspectives and experiences of Black women. In general, the world tends to dismiss our pain and viewpoints, so we don’t need the people who are meant to help us falling into that cycle.
Listening was described in terms of what is said but also not said by the therapist. Affirming their experiences, being empathetic, and understanding Black women’s lived experiences also seem connected to listening. Safe space and being genuine also seemed to be reflective of listening.
I think recognizing that Black women already have a lot on their plate and just being open to listening and being affirming in the process is invaluable. I don’t know that solutions should be pushed at the start, maybe it’s just important to have space for Black women to release.
Patience!!!! It will take time to uncover multiple layers of issues that impact us because historically we have been conditioned to ‘get over it’ and that attitude frames how we view our own incidents as well as how we choose to recall them.
1.5.6 Meta-Themes across All Responses
We analyzed participant statements to all four questions for meta-themes: overarching themes represented powerfully, frequently, and richly throughout respondents’ statements. We identified four meta-themes that seem to affect Black women’s experience of psychotherapy:
1. Cultural competence in therapists. This was a core and nonnegotiable feature of therapy for Black women that affected their capacity to trust and respond to therapy and therapists in several domains.
2. Cultural comfort in therapy. This theme is related to how Black women felt in therapy and with therapists. If women were comfortable that they were safe, seen, and understood culturally, they were more apt to trust the process and lean into the therapists’ ideas and suggestions.
3. Listening. This theme described a type of encounter led by therapists in which Black women felt validated, heard, understood, and accepted. These encounters increased women’s appreciation for the therapist and helped them to use therapy well. On the flip side, if therapists did not display listening, Black women seemed less apt to find therapy useful.
4. Time and cost of therapy. Multiple, intertwined meanings were attached to the cost of doing therapy. Costs were financial, cultural, social, personal, and the like. Cost often had the connotation of a price or penalty for doing therapy or having it not be successful. Related to cost was a sense that therapy was time consuming, and respondents noted alternative costs, such as just leaving things alone. References to time were not just in terms of minutes and hours but also opportunities lost and how negative experiences with one therapist may prevent a positive outlook on therapy itself. Our data suggest that the most consequential cost of therapy for Black women seems to be giving up on therapy altogether.
1.6 How Findings Relate to Ideas in the Book
Our study provides a snapshot of the viewpoints of Black women in our sample at the time of data collection. We cannot draw direct causal inferences, and we could not follow up with participants because of the anonymous nature of the survey. Nonetheless, these data, which nearly 800 individual statements by Black women, provided a wealth of insight into women’s perspectives on therapy, both from their own experiences and their perceptions of Black women’s experiences overall. Many themes in the data confirm the importance of the topics (see chapter titles) that we have included in this book. We should also know that while many topics we have selected are richly represented in the extant literature, there are some topics for which there are scant data as to the everyday experiences of Black women. This represents an opportunity for scholarly inquiry.
See titles and descriptions of each chapter in the Introduction.
In summing up the findings of the qualitative data, we note first, that while Black women may feel more comfortable with Black therapists, therapist race and gender alone are insufficient to gain women’s trust, and therapists must be willing to attend to cultural features of alliance building. Attention to Black women’s cultural comfort in therapy includes creating a safe space for them, showcasing interest and curiosity in Black women as a unique cultural group, showcasing cultural knowledge, and having information on the issues that affect Black women uniquely. Second, the study identified recurring themes connected to Black women’s core mental health conditions. In chapters of this book we have offered some information on why and how these themes might show up in Black women’s narratives. Recurring themes include the Strong Black Woman persona, shifting, family life, trauma, spirituality, mothering, and caregiving among others. Finally, the findings of our study endorse a need to build therapy relationships with Black women that are culturally competent. In several chapters of the book we will return to this theme and offer specific culturally competent strategies to gain Black women’s trust. The overall aim is to help therapists work with women’s needs in the contexts of their historical, social, and cultural experiences.
1.7 How the Study Impacts Our Practices
We learned a lot from our study that will alter aspects of our practice as therapists, and we hope therapists who read this work will find the same to be true for them. For example, Donna was especially struck by the fact that Black women are willing to give therapy a try despite not having their preferred option of a Black therapist. When Donna cannot accept a referral of a Black woman reaching out to her for therapy, she tends to refer the woman to another Black therapist in deference to the woman’s request. This has often delayed Black women’s ability to be in therapy simply because no Black therapists were available. Results of the study suggest an opportunity to encourage Black women to stick with their search for therapy and to consider culturally competent non-Black therapists among their options. Donna will incorporate such advice in making referrals.
Adia was struck by the number of issues Black women endorsed as contributing to their everyday stress. Adia views these stressors as related to Black women’s wellness overall, including physical health. She is considering outreach strategies to provide Black women additional therapy options as well as psychoeducation (e.g., targeted workshops on managing racism stress or group-based therapy services). Essential to this idea will be outreach efforts targeting women in community settings (e.g., churches).
Our three RAs also offered their views on the impacts of the study on them as therapists in training. We provide their comments here to honor their work and show how the themes identified in the study can influence the approach of developing therapists.
Sydney McClure, a Black female therapist in training, addresses the importance of clients’ safety in therapy:
What stands out for me that makes therapy helpful is having a “safe space.” While some study participants did not feel the need to elaborate on this quality, the qualities of a safe therapeutic space came through in other answers. The safety of therapy came from being a judgment-free zone. The therapist, especially if you are not Black, has to be trustworthy. However, many Black women might be slow to trust, especially. A safe space also means feeling connected with the therapist, feeling seen, feeling heard while not being interrupted or talked over. A safe space is one in which Black women can show vulnerability and be validated. Black women are asking therapists to not rush them, to consider all of their identities, to make time for them, to give them grace, to give them respect, to give them space, to provide them with tools, to listen, to see them, to hear them. Black women want therapists to show them the care and respect and empathy and care that almost every other space in our world does not grant Black women. Overall, I hope that when therapists read these results of this survey, they will feel it necessary to take action.
Katie Gow, a White female therapist in training, reflects on the deep importance of clients feeling understood and the need for therapists to reflect on their own position and reactions:
Engaging with these data has stirred up a variety of thoughts and feelings in me. The most troubling notion standing out to me relates to Black women’s fears, expectations, and experiences of being misunderstood. One woman writes that Black women may avoid therapy due to “feeling unheard and thinking a therapist’s office would be more of the same.” Another notes that avoidance may result from “not having their daily lived experiences understood or even explored by the therapist.” It would be a disappointing environment where, implicitly or explicitly, a therapist communicates that a Black woman’s life and experiences are not valued or worth seeing.
As I have thought about my privilege (as a White therapist) and consider what might get in the way of my ability (and perhaps others) to truly see and hear Black women, I think about a willingness to sit in discomfort. My privilege allows me to disengage from the reality of oppression when it feels like too much. I will need to consciously recognize when I feel an inclination to distance myself out of discomfort or feeling overwhelmed, to let myself feel what it means to live in Black women’s world. I hope not to minimize or fix or avoid the full experience in any way. This will require continuous work around recognizing the racism within me and my “white saviorism” and any tendency to protect myself and my comfort at Black women’s expense. I am incredibly grateful that this work is being done to serve them.
Finally, Lyrra Isanberg, a biracial therapist in training, shares concern and frustration in addition to hope for the future of the mental health profession:
As a biracial therapist-in-training (with Black ancestry) my initial response was worry. When I seek therapy for myself, are these experiences of discrimination, stereotyping, and microaggressions going to happen to me, too? It is difficult to understand that therapists with whom we do not share similar lived experiences can cause harm because of their ignorance. In some ways, I was greatly disappointed in this field after reading participants responses. However, I hope that reading about what Black women want such as listening, humility, and curiosity will be heard by present and future mental health workers who pick up this book. These responses renewed my understanding of the importance of taking proper heed to the need to correctly serve Black female clients.
Therapist Reflection Questions
1. How would you respond to the survey questions mentioned in this chapter?
2. What was new or surprising to you about the study findings? How might you change your clinical practice as a result?
3. As a therapist working with Black women what resonated with you? How might you use the ideas in this chapter to improve your practice with Black women?
4. As a student training to become a therapist, what aspects of this chapter did you find helpful? What will you want to know more about work related to Black women?
5. As a client in therapy, how do the ideas in this chapter help you to advocate for what you want?