



Impact statement
This scoping review highlights the importance of tailored interventions for migrants and ethnic minorities confronted with specific mental health challenges. Our findings provide valuable insight for healthcare policy-makers, local governments and scientific experts. Studies report high prevalence of mental disorders among these population groups. At the same time, structural and sociocultural barriers limit their access to mental healthcare and prevention. Therefore, the need for tailored interventions is high. This scoping review analysed 27 selected studies to identify what works in successfully promoting the mental well-being, and in preventing or dealing with mental health problems among migrants and ethnic minorities. This is the first comprehensive review that also identifies underlying intervention mechanisms leading to effective outcomes: (1) using a sound theory base, (2) systematically adapting the intervention in a culturally sensitive manner, and (3) the use of participatory approaches, preferably early on in their development. Our findings also point to the importance of holistic approaches addressing social health determinants to reduce mental health inequities. The findings and conclusions from this research should be used as guidance for the development of mental health interventions for diverse groups of migrants and ethnic minorities to make them more effective and sustainable.
Introduction
Migrant and ethnic minority populations are at greater risk for mental health problems than the general population in Europe and the European Economic Area (EU/EEA) (Carta et al., Reference Carta, Bernal, Hardoy and Haro-Abad2005; Fazel et al., Reference Fazel, Wheeler and Danesh2005; Missinne and Bracke, Reference Missinne and Bracke2012; Ekeberg and Abebe, Reference Ekeberg and Abebe2021; Purgato et al., Reference Purgato, Richards, Prina, Kip, Del Piccolo, Michencigh, Rimondini, Rudi, Vitali, Giovanni Carta, Morina, Schena and Barbui2021). While it has been suggested that some groups of migrants in certain contexts may have a health advantage over nationals upon their arrival (Dhadda and Greene, Reference Dhadda and Greene2018), this “healthy-migrant effect” appears to vanish with longer duration of residence due to increasing health inequalities. Evidence for migrants’ decline in mental health over the years is convincing (Elshahat et al., Reference Elshahat, Moffat and Newbold2021). Several studies show a higher prevalence of mental disorders such as post-traumatic stress disorder (PTSD), anxiety and depression among these populations, as well as of substance abuse and severe mental illnesses, such as psychosis in comparison with the majority population in the countries of residence (Fazel et al., Reference Fazel, Wheeler and Danesh2005; Missinne and Bracke, Reference Missinne and Bracke2012; Nosè et al., Reference Nosè, Ballette, Bighelli, Turrini, Purgato, Tol, Priebe and Barbui2017; Turrini et al., Reference Turrini, Purgato, Ballette, Nosè, Ostuzzi and Barbui2017; Foo et al., Reference Foo, Tam, Ho, Tran, Nguyen, McIntyre and Ho2018; Hynie, Reference Hynie2018; Ekeberg and Abebe, Reference Ekeberg and Abebe2021).
Migration trajectories and integration processes tend to be a psycho-social process of loss and change, associated with several mental stressors and suffering (Bhugra, Reference Bhugra2004; Carta et al., Reference Carta, Bernal, Hardoy and Haro-Abad2005; Derr, Reference Derr2016). Migration drivers such as poverty, violent political conflicts, and climate-related disasters will continue to trigger global migration (O’Malley, Reference O’Malley2018). The complex and interrelated combination of social and structural determinants pre-, during and post-migration impact migrants’ mental health (International Organization for Migration, 2006; Spallek et al., Reference Spallek, Zeeb and Razum2011; World Health Organization, 2022). Difficult socio-economic circumstances in their countries of origin such as limited access to education, employment and healthcare, economic disruptions, individual or family-related stressors might have affected their health status prior to and upon migration (Davies et al., Reference Davies, Basten and Frattini2010; Priebe et al., Reference Priebe, Giacco and El-Nagib2016). Migrants may face many challenges before and during their migration trajectory: some migrant groups are exposed to violence and trauma, often in the form of human rights violations (Priebe et al., Reference Priebe, Giacco and El-Nagib2016; Lindert et al., Reference Lindert, Schouler-Ocak, Heinz and Priebe2008; Purgato et al., Reference Purgato, Richards, Prina, Kip, Del Piccolo, Michencigh, Rimondini, Rudi, Vitali, Giovanni Carta, Morina, Schena and Barbui2021). After arrival, resettlement stressors, such as difficult socio-economic and living circumstances, complex legal residence procedures, detention procedures, and experiences of discrimination and racism, among others, may negatively affect their mental health (Priebe et al., Reference Priebe, Giacco and El-Nagib2016; Lindert et al., Reference Lindert, Schouler-Ocak, Heinz and Priebe2008; Nosè et al., Reference Nosè, Ballette, Bighelli, Turrini, Purgato, Tol, Priebe and Barbui2017; Von Werthern et al., Reference Von Werthern, Robjant, Chui, Schon, Ottisova, Mason and Katona2018).
Similar mental health vulnerabilities have been observed among ethnic minorities born in European countries (Myers, Reference Myers2009; Spallek et al., Reference Spallek, Zeeb and Razum2011; Borrell et al., Reference Borrell, Palencia, Bartoll, Ikram and Malmusi2015; Ikram, Reference Ikram2016; Hynie, Reference Hynie2018). The social determinants that impact migrant’s health before, during and after migration may also affect their offspring and subsequent generations (Spallek et al., Reference Spallek, Zeeb and Razum2011). Different genetic factors, cultural beliefs and health behaviours persist over generations, and the socio-economic conditions of parents can determine the health situation of their children (Spallek et al., Reference Spallek, Zeeb and Razum2011). Migrant descendants show a greater likelihood of developing mental disorders such as PTSD, as trauma can be transmitted to later generations through psychosocial mechanisms within the parent–child attachment and intra-family communication style (Sangalang and Vang, Reference Sangalang and Vang2017; Silwal et al., Reference Silwal, Lehti, Chudal, Suominen, Lien and Sourander2019). The complex issue of trauma transmission is not limited to family ties. Also, indirect experiences of racial discrimination, racial profiling, and racism were shown to affect the mental well-being among some ethnic minority groups (Cénat, Reference Cénat2020).
The evidence on the particular causes and circumstances of migrant groups’ heightened vulnerabilities to ill mental health, gives reason for specific, targeted interventions on mental health promotion, prevention, and treatment, apart from interventions targeting the general non-migrant and/or ethnic majority population (Uphoff et al., Reference Uphoff, Robertson, Cabieses, Villalón, Purgato, Churchill and Barbui2020). Migrants and ethnic minorities might experience language, cultural and structural barriers that complicate access to regular mental healthcare (Uphoff et al., Reference Uphoff, Robertson, Cabieses, Villalón, Purgato, Churchill and Barbui2020) and thus they may make less use of health care services or use services in a different manner (Graetz et al., Reference Graetz, Rechel, Groot, Norredam and Pavlova2017). Most of the target-group specific interventions on mental health, however, seem to be directed to the specific subgroup of refugees and asylum seekers, who have specific needs given their specific migration history, distinct legal status, and access to health systems (Nosè et al., Reference Nosè, Ballette, Bighelli, Turrini, Purgato, Tol, Priebe and Barbui2017; Lebano et al., Reference Lebano, Hamed, Bradby, Gil-Salmerón, Durá-Ferrandis, Garcés-Ferrer, Azzedine, Riza, Karnaki, Zota and Linos2020; Uphoff et al., Reference Uphoff, Robertson, Cabieses, Villalón, Purgato, Churchill and Barbui2020; Purgato et al., Reference Purgato, Richards, Prina, Kip, Del Piccolo, Michencigh, Rimondini, Rudi, Vitali, Giovanni Carta, Morina, Schena and Barbui2021). An overview of interventions focusing on refugees and asylum seekers can be found in the Cochrane Library (Uphoff et al., Reference Uphoff, Robertson, Cabieses, Villalón, Purgato, Churchill and Barbui2020) and further in this special issue to be published in the journal. Other migrant groups, such as economic migrants, as well as ethnic minorities who are subject to similar mental health risks, are not considered in those reviews.
Additionally, intervention reviews rather focus on those populations already diagnosed with a mental health condition and little emphasis is put on the prevention of mental health problems or promotion of mental well-being in those groups at increased risk (Purgato et al., Reference Purgato, Richards, Prina, Kip, Del Piccolo, Michencigh, Rimondini, Rudi, Vitali, Giovanni Carta, Morina, Schena and Barbui2021). However, prevention strategies and mental health promotion approaches are essential to ensure psychological well-being, reduce the mental health burden as well as to improve the mental health outcomes of migrant and ethnic minority groups (Foo et al., Reference Foo, Tam, Ho, Tran, Nguyen, McIntyre and Ho2018). While it is clear that migrants and ethnic minorities are exposed to various risk factors, this exposure does not necessarily lead to the development of mental health problems. Resilience factors, such as social support, positive coping strategies, and personal characteristics can help individuals navigate adversity and prevent mental health problems to develop (Dubus, Reference Dubus2022). Resilience can also be fostered through utilising available resources to address mental health concerns. Therefore, interventions that focus on increasing resilience, such as by strengthening social networks, may help to prevent mental health problems among migrants and ethnic minorities.
In the current literature, no review could be found on mental health interventions for the broader group of migrants and ethnic minority populations in Europe. The existing review studies on refugees and asylum seekers are particularly relevant to shed light on these groups’ specific needs, recognising the fact that forced migration may constitutes the highest mental health risk (Uphoff et al., Reference Uphoff, Robertson, Cabieses, Villalón, Purgato, Churchill and Barbui2020). However, we also need a better understanding of what renders mental health interventions effective for the larger group of migrants and ethnic minorities. This includes a broad range of people such as first-generation migrants (which may or may not include previous refugee experiences), second-generation migrants and ethnic minorities. Recognising the fact that no universally accepted definition of migrants exists (IOM, 2023), the current scoping review uses the International Organisation for Migration definition of migrants (IOM, 2019) “as anyone who moves away from their usual place of residence regardless of legal status, the reason for migration and the length of stay.” This review aimed to fill the above-mentioned knowledge gaps for this broader groups of migrants and ethnic minorities as population of interest by mapping and synthesising the available evidence on effective approaches and interventions to improve their mental health and well-being.
Methodology
A scoping review methodology was fit for the purpose given the broad field of inquiry and the likely mix of outcomes and research designs adopted. We applied Arksey and O’Malley’s multistage methodological framework (Arksey and O’Malley, Reference Arksey and O’Malley2005), taking into account Levac et al.’s (Reference Levac, Colquhoun and O’Brien2010) refinements. The stages are: (1) Clarifying and linking the purpose and research question, (2) Identifying relevant studies and balancing feasibility with the comprehensiveness of the scoping process, (3) Applying an iterative team approach in the study selection, (4) Charting the data, and (5) collating and summarising the results through a qualitative thematic analysis and reporting implications of the findings for policy, practice and research. The systematic data selection was based on the PRISMA extension guidelines for scoping reviews (Tricco et al., Reference Tricco, Lillie, Zarin, O’Brien, Colquhoun, Levac, Moher, Peters, Horsley, Weeks, Hempel, Akl, Chang, McGowan, Stewart, Hartling, Aldcroft, Wilson, Garritty, Lewin, Godfrey, Macdonald, Langlois, Soares-Weiser, Moriarty, Clifford, Tunçalp and Straus2018).
Stage 1: Clarifying and linking the purpose of the review to the research question
Definitions
The term “Migrants and ethnic minorities” describes heterogeneous groups with numerous definitions. For this study, we used the definitions of the International Organization for Migration (IOM) (2019). In this framework, “migrant” is defined as “an umbrella term, not defined under international law, reflecting the common lay understanding of a person who moves away from his or her place of usual residence, whether within a country or across an international border, temporarily or permanently, and for a variety of reasons.” “Ethnic minority groups,” are in this scoping review broadly defined as a group within a community that has a specific way of life, based on meanings, crucial for processes of identification and differentiation (Jenkins, Reference Jenkins2008), which differs from the rest of the population. In many cases, but not always, ethnicity is intertwined with migration, increasing their significance and salience, which makes it also interesting to discuss together in this review (Erel et al., Reference Erel, Murji and Nahaboo2016).
To inform the further scoping process, we delineated the scope of the search, operationalised the search terms and defined a clear research question (Levac et al., Reference Levac, Colquhoun and O’Brien2010). During a first team meeting, we discussed and decided on the research question based on a PICo approach (Population, Interest and Context) (Stern et al., Reference Stern, Jordan and Mcarthur2014; Eriksen and Frandsen, Reference Eriksen and Frandsen2018; see Table 1). The protocol has been registered at the Center for Open Science (https://doi.org/10.17605/OSF.IO/R8SBF).
Table 1. Delineating the review question and refining the search strategy based on PICo-approach

The conceptualization of these terms led to a clearly articulated scope of inquiry and enabled us to develop the following research question for the review:
What is known about interventions applied in the EU/EEA +UK to improve migrants’ and ethnic minorities’ mental health or well-being?
Building further on this general review question, we defined the following specific objectives: (1) To identify what interventions are available and their respective outcomes; (2) To provide an overview of the intervention mechanisms and culturally adapted delivery strategies applied within the selected studies, focusing on the specific target groups; and (3) To identify barriers and facilitators for intervention uptake. Finally, the goal of this scoping review is to give recommendations for policy and practice based on the critical appraisal of the available evidence.
Stage 2: Identifying relevant studies
We added eligibility criteria for the search strategy to the PICo-criteria, such as year of publication, availability of text and language of publication. We searched for peer-review journal articles available in full-text and written in English until the date of the search, that is, 01/07/2022. We included all study designs. We excluded comments, letters to the editor, books and book chapters, conference abstracts and theses. We defined the search terms and potential databases, based upon available resources by the review team (i.e., consisting of the first three authors). The first author conducted a few try-out literature searches using different databases to check for the most suited search terms and date range. Interim results were continuously discussed by the team to develop the final, comprehensive search string. We searched three main relevant bibliographic databases from their inception, that is, PubMed, Web of Science and PsycInfo. Key search terms were a combination of the core concepts of our research objectives and related terms or synonyms. The core concepts were “intervention,” “improving,” “mental health,” “migrants and ethnic minorities” and “countries from EU/EEA + UK.” The fully applied search strings can be found in the Supplementary Material.
Stage 3: Study selection
All results of the final literature searches were deduplicated using EndNote and were listed by the first author in a Microsoft Excel file. The first three authors screened the results (title and abstract) independently. During several team meetings, they discussed all results and selected relevant studies for full-text reading according to the eligibility criteria (as listed in Table 1). Reasons for exclusion after full-text reading were reported and categorised. If full-text reading revealed reference to other relevant articles, not included in the search results, an additional manual search was performed to include and assess those studies. Furthermore, we have scoped the individual studies within the meta-analyses. Most studies were also retrieved by our own search strategy. However, studies that met our inclusion criteria, were additionally included (e.g., Jacob et al., Reference Jacob, Bhugra and Mann2002; Chaudhry et al., Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009). Furthermore, we included the meta-analyses as well, as we deemed their analyses and comprehensive conclusions relevant for answering our review questions and the discussion of the results. The flowchart in Figure 1 illustrates the details of the search and selection process.

Figure 1. Flowchart of search and selection process.
Stage 4: Charting the data
The first author drafted a data extraction sheet using Microsoft Excel, which was piloted by the team with several articles. The data extraction sheet compiled the following key characteristics of the full-text articles: author, year of publication, title, country of study, participant characteristics, sample size (if applicable), methodological approach and study design, context of study, phenomenon of interest, theory of change (if applicable), intervention description, used instruments to measure outcomes, results and outcomes, barriers, facilitators, recommendations, study limitations, and data screeners’ remarks. Reasons for exclusion after full-text reading were recorded. All selected articles were randomly assigned to one of the three first authors to extract data, and cross-checked and discussed with the other team members. The categories used in the data extraction sheet form the basis for the next steps, that is, the synthesis of the results.
Stage 5: Collating and summarising the results
We performed a thematic narrative synthesis of the selected articles to analyse the relevant thematic, methodological, and population-specific characteristics. We first inductively coded the intervention relating to their content (see the descriptive part under results). We then mapped the identified interventions along a continuum of disease prevention (i.e., primary prevention and promotion of well-being to prevent problems before they emerge) to secondary prevention (i.e., targeted interventions for people at high risk of developing mental disorders when exposed to specific risk factors) to tertiary prevention (i.e., focusing on interventions for people with acute or chronic mental health problems). The latter is distinct from pharmacological treatment (see eligibility criteria) but focusing on strategies to support patients in coping and living well with ill mental health including self-management. While we acknowledge that these stages may overlap and fluctuate in real life (Purgato et al., Reference Purgato, Richards, Prina, Kip, Del Piccolo, Michencigh, Rimondini, Rudi, Vitali, Giovanni Carta, Morina, Schena and Barbui2021), we use them for theoretical conceptualisation and because many health professionals are familiar with it. Clearly, this categorisation remains descriptive, and does not address underlying health disparities relevant for migrant mental health based on, for example, ethnic inequities or socio-economic status, as indicated by Compton and Shim (Reference Compton and Shim2020). Instead, Compton and Shim (Reference Compton and Shim2020) propose to look at how to reduce the population burden of social mental health determinants, which are highly interconnected. A true classification system for mental health interventions based on social determinants of health does not exist. We therefore aimed to contribute to this theoretical gap by analysing the intervention mechanisms in terms of addressing the different levels of social health determinants.
To provide accurate answers to the research objectives, we also analysed the intervention approaches used in-depth. For instance, we analysed the category “intervention description” with a specific focus on the interventions’ cultural adaptation. Similarly, interventions describing a participatory approach, were labelled under different categories along the continuum proposed by Attygalle (Reference Attygalle2020): from community-informed (CI) over community-shaped (CS) interventions to community-driven (CD) initiatives. Interventions aiming to increase access to services at the respective stages of the prevention continuum were also included.
All authors commented on all results, conclusions drawn, and policy recommendations made and achieved consensus through discussion.
Results
Description of selected studies
We retrieved 282 results in PubMed starting from 1989, 253 results in Web of Science from 1993 and 99 results in PsycInfo from 2012. After the removal of duplicates and the screening process, we included 27 articles in the final selection, covering a period between 2002 and 2022. An overview of the studies can be found in Table 2. The number of articles and the number of interventions differ, as two articles, that is, Osman et al. (Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017, Reference Osman, Vixner, Flacking, Klingberg-Allvin, Schön and Salari2021) focus on the same intervention/program. We have included both articles as they describe relevant information on the intervention’s mechanisms and results. The majority of the literature was published after 2010 (n = 20), with the number of articles peaking in 2015 (n = 3), 2017 (n = 4), and 2021 (n = 4). The selected articles comprised quantitative (n = 9), mixed methods (MM; n = 9), qualitative studies (n = 6), and review studies (n = 3; one scoping review and two meta-analyses), as shown in Figure 2. Among the quantitative studies, the majority were intervention studies describing randomised controlled trials (RCT) (n = 8), and one observational pre-and post-test design of a pilot study. The MM studies included n = 2 (exploratory) randomised trials with an embedded qualitative component using interviews and focus groups to assess participants’ experiences with the respective interventions. Two MM studies adopted a longitudinal cohort design combining quantitative with qualitative data. The qualitative studies adopted different study designs (i.e., a case study, interview studies (n = 3) and qualitative evaluations of pilot studies (n = 2)). The majority of the studies described interventions in a single country, that is, the UK (n = 13), the Netherlands (n = 5), Sweden (n = 3), and Ireland (n = 1). Four studies focused on multiple countries or had a global scope including Europe.
Table 2. Overview of intervention studies – Alphabetical order

Abbreviations: AoR, arts-on-referral; BME, black and minority ethnic, British ethnic minority population; CaFI, culturally adapted family intervention; CBT, cognitive behavioural therapy; CI, confidence interval; EPDS, Edinburgh postnatal depression scale; EQ-5D, European quality of life – 5 dimensions; FI, family intervention; FSM, family support members; FU, follow-up; GHQ-28/12, general health questionnaire (28/12 items); GP, general practitioner; GSH, guided self-help; HADS, hospital anxiety and depression scale; HMHB, “happy mothers, happy babies”-programme; HRSD, Hamilton rating scale for depression; MADRS-S, Montgomery–Asberg depression rating scale; NHS, National Health Service; OR, odds ratio; PHP, positive health program; PCM, participation chain model; PHQ-9, patient health questionnaire; PTSD, post-traumatic stress disorder; RCT, randomised controlled trial; SCAN, schedule for clinical assessment in neuropsychiatry; SD, standard deviation; SF-36, short form survey (36 items); SIDS, sudden infant death syndrome; SRQ, self reporting questionnaire; TAU, treatment as usual; WEMWBS, Warwick Edinburgh mental well-being scale; WSAS, work and social adjustment scale.

Figure 2. Countries, methods used and intervention content of the included studies.
In terms of intervention content, we first categorised the interventions inductively based on their main intervention content, independent of setting or delivery modes. This resulted in the following distribution: five articles reported on parenting programs (including pre,- peri- and postnatal programs), nine articles on social change intervention in the wider sense, three on lifestyle intervention (physical activity), two on arts-based interventions, three on self-help interventions (of which two were e-health interventions), and two on health education interventions. Looking at when in the course of prevention these interventions were delivered, we classified eight as primary prevention, eight as secondary, and nine as tertiary prevention (see Table 3).
Table 3. Categorisation of studies

Abbreviations: CD, community-driven; CI, community-informed; CS, community-shaped.
Population groups
The selected studies addressed a wide variety of population groups and differed in the terminology used to characterise the study population. Studies mainly from the UK addressed Black and Ethnic Minority (BME) populations (Knifton et al., Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014; Rabiee et al., Reference Rabiee, Robbins and Khan2015; Van de Venter and Buller, Reference Van De Venter and Buller2015; Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017). Others addressed people of African and Caribbean origin (Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010; de Freitas and Martin, Reference de Freitas and Martin2015; Mantovani et al., Reference Mantovani, Pizzolati and Gillard2017; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018). Several studies focused on target groups by nationality, such as Turkish (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008; Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), Moroccan (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008), Pakistani (Chaudhry et al., Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009; Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019), Indian (Jacob et al., Reference Jacob, Bhugra and Mann2002), Somali (Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017, Reference Osman, Vixner, Flacking, Klingberg-Allvin, Schön and Salari2021), and Iraqi migrants (Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019). One qualitative study focused on forced migrants of different origins in a global perspective, including Germany, Greece and Switzerland (Dubus, Reference Dubus2022). We excluded studies solely focusing on asylum-seekers and refugees, however, this study included participants with undocumented residence status next to refugees and asylum-seekers. Three studies included both ethnic minority populations as well as service providers and institutional stakeholders to assess and triangulate their different perspectives as research participants (de Freitas and Martin, Reference de Freitas and Martin2015; Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017; Dubus, Reference Dubus2022). Two intervention studies were inclusive interventions, targeting socially disadvantaged and underserved populations including ethnic minority populations, yet providing disaggregated results (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014; Van De Venter and Buller, Reference Van De Venter and Buller2015). Finally, 6 intervention studies were developed and tested exclusively for ethnic minority women (Jacob et al., Reference Jacob, Bhugra and Mann2002; Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008; Chaudhry et al., Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009; Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010; Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019). The three review studies applied a broad definition of target populations, and included a combination of different ethnic minority populations. One study (Baskin et al., Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021) focuses on UK minority populations, using ethnicity descriptors as defined by the UK 2011 Census from the Office of National Statistics (Office for National Statistics, 2011). Applying the same descriptors in combination with those from the United States Census Bureau (United States Census Bureau, 2020), Arundell et al. (Reference Arundell, Barnett, Buckman, Saunders and Pilling2021) enlarged their focus to “black, ethnic minority, migrant, refugee or asylum seeker communities, and people referred to as ‘minorities’ or defined as belonging to an identified racial or ethnic ‘minority group’” in their global review. Degnan et al. (Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018) used the broad definition of ethnic group or subculture, being “a minority culture within a larger dominant culture.”
Types of interventions
Using a public health lens, we describe the identified studies on a prevention continuum, as presented above (see Table 3). Two studies were labelled within multiple categories, for example, an intervention combining evidence-based treatment approaches with mental health promotion at the community level (Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021; Dubus, Reference Dubus2022).
Primary prevention and promotion of well-being
We classified eight studies as primary prevention interventions. Given the economic advantages as well as the legal and human right obligations to keep migrants and ethnic minority populations healthy (Agyemang, Reference Agyemang2019), interventions that support them in maintaining good mental health are relevant. The identified interventions were quite diverse in terms of their approaches used, intervention strategies, and target populations. Studies were either based on thorough cultural adaptation of already existing evidence-based interventions, such as a Dutch study reporting on the successful cultural adaptation of a physical exercise program for elderly Turkish migrants in the Netherlands (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003). The intervention resulted in significant mental health improvements, but not in physical well-being and exercise activity (see Table 2). An exploratory primary care trial tested a well-being intervention in general practitioners (GP)-settings in the UK (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014) including both underserved older Europeans and people of Somali- or South Asian origin. This intervention combined individual- and group elements with adequate referral and resulted in improved well-being and social functioning in both groups. However, community engagement turned out to be a more relevant factor in the migrant group than in the comparison group. Three studies described community-led interventions emphasising participatory approaches (Knifton et al., Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010; Malone et al., Reference Malone, McGuinness, Cleary, Jefferies, Owens and Kelleher2017; Mantovani et al., Reference Mantovani, Pizzolati and Gillard2017). The latter used arts-based strategies to engage communities, while Mantovani et al. (Reference Mantovani, Pizzolati and Gillard2017) adopted a community engagement model to train and work with well-being champions. Earlier, Knifton et al. (Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010) engaged community members to hold awareness-raising workshops effectively addressing mental health stigma and discrimination. A culturally sensitive perinatal program systematically developed for pregnant Turkish mothers (“Healthy mothers, healthy babies”) engaged ethnic minority midwives to conduct group sessions and home visits (Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012). The intervention delivered in mother–child centres demonstrated a positive effect for mild depressive symptoms, but was underpowered to detect differences in other envisaged outcomes (i.e., severe depression, parenting behaviours, smoking cessation).
Secondary prevention
Eight articles qualified as targeting people and groups who are at heightened risk of developing mental health problems. The mental health and psychosocial problems addressed differed according to studies and targeted populations. Conditions and population groups addressed included PTSD among forced migrants of diverse origins in a multi-country study using a resilience approach (Dubus, Reference Dubus2022), acculturation stress among Somali-born parents in Sweden (Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017, Reference Osman, Vixner, Flacking, Klingberg-Allvin, Schön and Salari2021), concurrent diabetes and depression among Iraqi immigrants in Sweden (Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019), suicidal ideation among Turkish migrants in the Netherlands (Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), and psychosomatic problems and pain among Turkish and Moroccan women in the Netherlands (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008).
One study looked at access to mental health services for people diagnosed with mental illness (Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017) using co-production techniques. A qualitative study explored how Cape Verdean migrants experiencing psychosocial problems (de Freitas and Martin, Reference de Freitas and Martin2015) could be encouraged, valued, and sustained through participatory initiatives by creating community-based hybrid mental health spaces. A culturally adapted health education intervention delivered in primary care settings in the Netherlands used trained migrant educators providing culturally adapted information, counselling and support based on stress reduction theory for women of Turkish and Moroccan origin with psychosomatic problems (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008). The randomised controlled trial showed significant improvements in perceived general and psychological health, and self-reported ability to cope with pain in the intervention group compared to a control group receiving treatment as usual (TAU). No effects were found on social support and the perceived burden of stressful life events due to precarious life circumstances. The evaluation revealed participants’ subjective perceptions of psychosomatic problems due to their different explanatory mental health models, as well as difficulties to change social support from the women’s environment due to their often difficult socio-economic situation.
Tertiary prevention and self-management
We identified nine articles focusing primarily on tertiary prevention. Since the continuum is fluid, two studies (Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021; Dubus, Reference Dubus2022) covered both secondary and tertiary prevention. Importantly, these studies showed how the use of migrant community health workers (e.g., Jacob et al., Reference Jacob, Bhugra and Mann2002; Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010; Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010) can help to target social determinants underlying mental health conditions. Studies were targeting families and social groups: two studies described family interventions: one study addressed women with postnatal maternal depression using cognitive-behavioural therapy (Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019), and Edge et al. (Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018) reported on a systematically developed family-based intervention for schizophrenia. Two studies reported on social group interventions (Chaudhry et al., Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009; Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010), the latter in a primary care setting. Two interventions trained and employed community health workers (Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010), or trained migrant health educators (Jacob et al., Reference Jacob, Bhugra and Mann2002). Finally, we identified two culturally adapted self-management interventions using online technologies. The online intervention by Eylem et al. (Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021) used culturally adapted elements of an already existing evidence-based e-intervention to reduce suicidal ideation coupling Cognitive Behavioural Therapy (CBT) with mindfulness practices. The intervention was evaluated using an RCT design with waiting-list control condition both in the UK and the Netherlands targeting Turkish migrants at risk of suicide. It showed improved suicidal ideation, depression, and hopelessness scores in both groups, no suicide attempt was reported during the study period, and participants reported better self-management. Participants perceived the mindfulness practices as helpful but reported that the online intervention provided too little structure while not being diversified enough. This pointed to the heterogeneity of migrant communities, and the existence of specific micro-identities. Another UK-based study (Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010) tested the feasibility and effectiveness of a culturally acceptable package of mental health care to improve the health and psychosocial functioning among BME patients, mainly of sub-Saharan African descent with a previous history of diagnosed depression and/or anxiety. Trained community health workers (i.e., ethnically matched psychology graduates) delivered brief CBT interventions under supervision), as well as advocacy and mentoring creating rapid access. This small-scale randomised community trial comparing an intervention group with TAU (i.e., local mental health services) showed significantly improved levels of depression at the 3 months follow-up for the rapid access group. It was the only study including a cost-effectiveness component, demonstrating that a needs-led mental health package did not significantly increase costs of service use. This intervention also improved the interface between statutory agencies and African community organisations, which is relevant from a policy point of view.
Intervention mechanisms: Possible pathways to effective intervention outcomes
Interventions’ effectiveness
Three reviews looked at the effectiveness of interventions (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021; Baskin et al., Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021). Two meta-analyses demonstrated significant improvements of culturally adapted interventions over time compared to non-adapted interventions: one systematic review including 46 studies with more than 7,800 participants looked at post-treatment effects of culturally adapted psychosocial interventions for patients living with schizophrenia. The review showed significant post-treatment improvements for total symptom severity over interventions that were not explicitly mentioned to be adapted for the specific cultural population groups (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018). A second systematic review (Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021) synthesised 88 studies describing psychological interventions for people belonging to ethnic minority populations experiencing or being diagnosed with a wide range of mental health problems (depression, anxiety, post-traumatic stress syndrome, psychosis, eating disorders and other non-specified mental health problems) on a global scale. The meta-analysis found medium effect size in reducing symptom severity in favour of adapted interventions when compared to controls, across all target conditions and adaptation types including self-help interventions. A narrative scoping review (Baskin et al., Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021) looked at the effectiveness of interventions using a community-centred approach in the UK. The authors identified seven studies, including four studies reporting statistically significant positive effects on mental health outcomes. Social connectedness, access to safe and affordable housing, and power in local decision-making were reported as important determinants for intervention effectiveness.
Among the studies identified in our review, several studies also showed significant improvements in mental health: six of the seven intervention studies adopting an RCT design demonstrated a positive effect on mental health outcomes, mostly a reduction in depression rates (Jacob et al., Reference Jacob, Bhugra and Mann2002; Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008; Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010; Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019). Also, a non-randomised trial study (Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012) showed positive effects on reduction of mild depressive symptoms.
This points to an increasing evidence-base of effective interventions, at least under the controlled circumstances of trial studies. Interestingly, the four lifestyle interventions focusing on regular physical activity to also improve mental health outcomes, were all able to demonstrate positive impact on mental health outcomes (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017, Reference Osman, Vixner, Flacking, Klingberg-Allvin, Schön and Salari2021; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019). Also, the pilot evaluation of a free access scheme to exercise facilities for BME communities in the UK showed a preliminary increase in energy levels and self-confidence as well as reduction in stress, depression and anxiety (Rabiee et al., Reference Rabiee, Robbins and Khan2015). These findings show that social and environmental circumstances are integral to lifestyle choices, hence the importance of public health policy to facilitate the joining up of different organisations to increase access and offer tailored activities.
Different factors explained why some interventions did not produce significant improvements on mental health outcomes, either referring to flaws in the study design or in the difficulty to impact structural and social factors. Some studies reported improvements in both intervention and control groups (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), showing the difficulty of conducting an RCT in real-life circumstances as community and social influences cannot be excluded (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013). Studies did not assess the exposure to usual care, provide sufficient cultural adaptation or assess mental health stigma (Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), or had problems recruiting sufficient participants (Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012). While direct support from migrant health educators contributed to the improved effects on coping and mental health, social support from participants’ direct personal environment as one of the determinants of mental health problems proved to be more difficult to be influenced (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008).
Theory-driven interventions and intervention mechanisms
We analysed the theory-driven processes underlying the interventions, and the hypothesised processes leading to the observed outcomes. Evidence shows that complex healthcare interventions are more likely to be effective, sustainable, and scalable if they are using a sound theory-base and describe and test the causal pathways through which an intervention may achieve its expected outcome (De Silva et al., Reference De Silva, Breuer, Lee, Asher, Chowdhary, Lund and Patel2014). Providing such information also makes the intervention replicable, increasing knowledge on both the interventions’ mechanisms and practical implementation. Against this background, we took a rather broad approach and coded whether studies provided any information on their underlying theory-base for assumed causal changes achieved through the intervention. Evidence also shows that developing, implementing, and evaluating interventions in collaboration with stakeholders adds to their effectiveness (Bartholomew et al., Reference Bartholomew, Markam, Ruiter, Fernández, Kok and Parcel2016). Thus, we also coded stakeholder participation (i.e., any pragmatic framework or narrative description explaining how the intervention may affect change).
More than half (n = 16) of the selected articles on intervention studies explicitly described their underlying theory base and hypothesised intervention mechanisms. Parenting interventions for instance, were based on attachment theory to support distressed parents in their adaptation to parenting styles in the host country change (i.e., Sweden) (Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017). For lifestyle interventions working with physical exercise, a combination of neuro-biological, psychological and social mechanisms was mentioned: enhanced physical activity leads to increased release of neurotransmitters believed to improve mental health, and psychological mechanisms such as social interaction and social support to improve self-esteem and self-efficacy (Rabiee et al., Reference Rabiee, Robbins and Khan2015; Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017). This resulted in self-empowerment, which indeed showed improved scores in depression outcomes among Iraqi immigrants from baseline to the 3 months follow-up (Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019). Some studies also focused on the improvement of communication patterns between mental health care providers and patients due to culturally diverse explanatory models, mainly through cultural mediators, community health workers and well-being champions (Jacob et al., Reference Jacob, Bhugra and Mann2002; Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008; Mantovani et al., Reference Mantovani, Pizzolati and Gillard2017).
Several interventions aimed at improving mental health outcomes through the creation of social networks to increase social contacts and activities in a culturally acceptable manner, therefore reducing social isolation. Combining such elements with psychoeducation to increase correct information on depression resulted in significant reduction of depression in a social intervention delivered in primary care settings for British Pakistani women with depression at 3 and 9 months follow-up (Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010). Chaudhry et al. (Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009) mentioned a similar theory of change: providing mental and physical health education and facilitating the development of informal networks to increase engagement in social contacts would reduce depression; they also linked the participants to appropriate mental health services to increase access. This intervention showed a significant reduction in depression scores from pre-to post-test, and feedback from the nine British Pakistani women with diagnosed depressive disorders showed that they perceived their relationship with the group session facilitators and the provision of transport as the most important components of the intervention. Some studies did not explicitly describe their underlying change models, but mentioned that they were systematically developed, or that they had conducted their own need assessment (Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018) or a cyclic process of data collection and evaluation (Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018). Specifically, Kocken et al. (Reference Kocken, van Zwanenburg and de Hoop2008) recommended using generic guiding frameworks for the systematic development of health promotion interventions, such as the intervention mapping protocol to effectively tailor interventions to migrants’ needs.
The underlying theory-base specifying the respective determinants that interventions aim to address to achieve the envisaged behavioural outcomes is also relevant as it determines the choice of the respective intervention strategies (Bartholomew et al., Reference Bartholomew, Markam, Ruiter, Fernández, Kok and Parcel2016): n = 7 intervention studies explicitly mentioned using cognitive behavioural therapy (CBT) approaches (Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010; Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021; Dubus, Reference Dubus2022) or strategies that used CBT elements, such as personalised goal setting. As there is a large body of evidence for the effectiveness of CBT in treating mental health conditions, some of these interventions were based on existing evidence-based interventions, which were culturally adapted (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), other studies developed new interventions using participatory approaches (Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010; Dubus, Reference Dubus2022). The second main strategy consisted of various peer-support and participatory strategies (n = 6) focusing on empowerment through the facilitation of social interaction and social support (Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010; Knifton et al., Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010; de Freitas and Martin, Reference de Freitas and Martin2015; Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017; Mantovani et al., Reference Mantovani, Pizzolati and Gillard2017; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019).
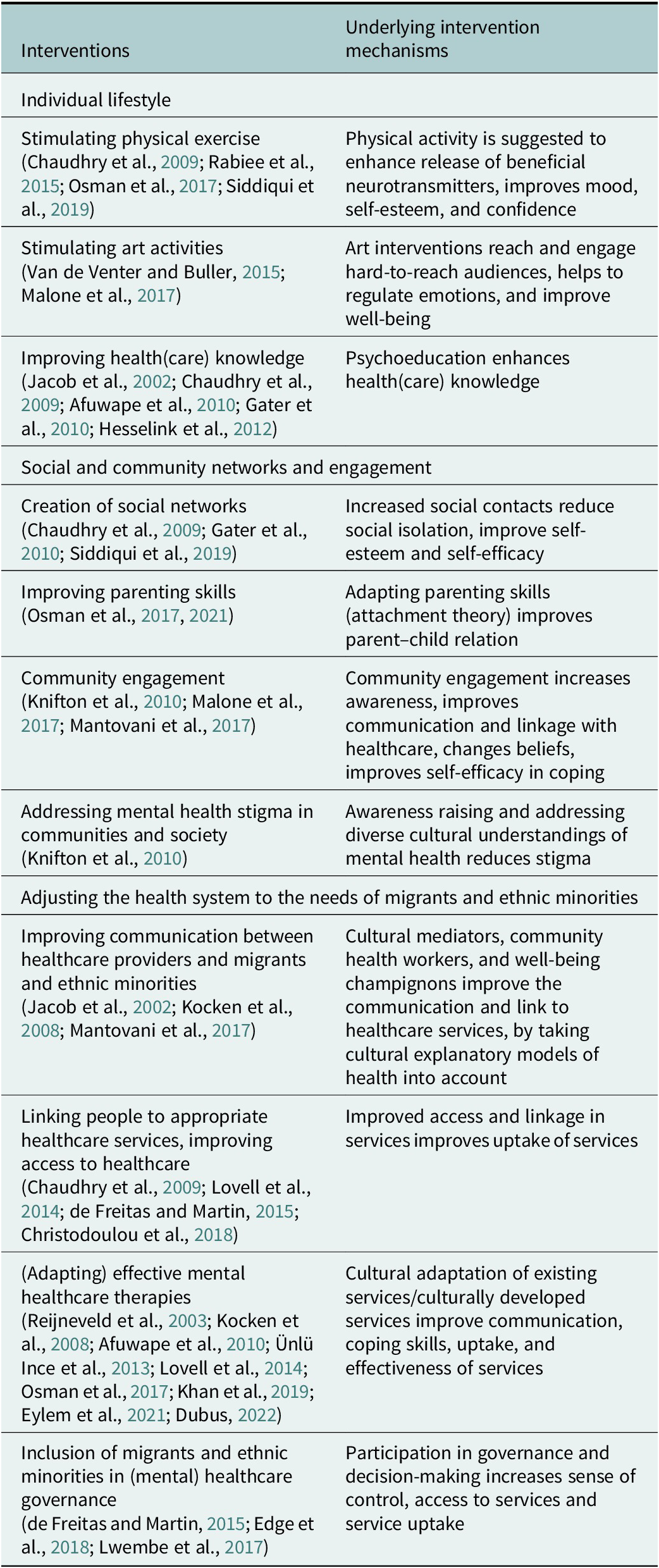
Table 4 summarises and ranks the different interventions and their change mechanisms (if mentioned in the studies) according to the level of social determinants they addressed: from the micro-level addressing individual level-factors, such as health education to change lifestyles, to interventions on the meso-level, focusing on migrants’ and ethnic minorities’ social and community networks, to interventions on a macro-level focusing on health systems changes through, for example, community participation and shared decision-making. We have adapted these levels from the often-applied social determinant framework, coined by Dahlgren and Whitehead (Reference Dahlgren and Whitehead1991). Some interventions addressed multiple levels of social determinants, for example, Gater et al. (Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010) created social networks and increased the participants’ knowledge on depression. For conceptual clarity, we distinguish between these levels, yet clearly they interact with each other and ultimately influence mental health at the individual level (Glanz et al., Reference Glanz, Rimer and Viswanath2008).
Table 4. Interventions and their underlying intervention mechanisms ranked according to different levels of social determinants
Cultural adaptation of interventions
In general, we could distinguish two types of studies: interventions based on a cultural adaptation of already existing evidence-based interventions and newly developed interventions specifically designed for a certain population group. Those studies adapting existing interventions in a culturally sensitive way did so to various degrees: ranging from the design of the intervention, as a feedback process, during the implementation, adjusting language and translation issues or dealing with the (socio-economic) preconditions to enable participation in the intervention. In addition, interventions were frequently adjusted to a specific culture or target group, taking into account local habits, languages and explanatory models.
Eight studies discussed the cultural adaptation of an existing intervention, see Table 3. As mentioned above, CBT approaches were modified for the specific target groups. Importantly, adopting CBT elements was independent of who delivered the intervention (e.g., expert patients as co-facilitators or professionals such as therapists or GPs) or in which type of setting, thus including e-health interventions (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), a CBT-based therapy (Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019) or a well-being program for primary care (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014). Osman et al. (Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017, Reference Osman, Vixner, Flacking, Klingberg-Allvin, Schön and Salari2021) based their intervention on the evidence-based parenting programme CONNECT, which they delivered using a culturally sensitive approach. In the study of Edge et al. (Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018), an existing family intervention was adapted by applying a participatory approach with African-Caribbean people diagnosed with schizophrenia, their families, service providers and researchers. Lifestyle interventions were adapted by Siddiqui et al. (Reference Siddiqui, Lindblad, Nilsson and Bennet2019), focusing on healthy lifestyle habits, and Reijneveld et al. (Reference Reijneveld, Westhoff and Hopman-Rock2003), who adapted a physical exercise program called “Healthy and Vital program.” In addition to these single studies, also two review studies discuss culturally adapted interventions (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021). Degnan et al. (Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018) focus on adapted psychosocial interventions for schizophrenia, assessing their effectiveness (see above) and proposing a framework for cultural adaptation. Arundell et al. (Reference Arundell, Barnett, Buckman, Saunders and Pilling2021) determined the effectiveness of cultural adaptations in psychological intervention for BME groups (see above) and developed a conceptual typology.
The strategies to culturally adapt interventions varied over the different phases of intervention studies, see Table 5. In a pre-development stage, preparatory focus group discussions with community members were held to identify adaptation needs (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018). In the process of intervention development, adaptations made included the (back)translation of intervention materials (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), modifications in content (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021) such as modifying concepts and including well-known idioms and metaphors (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), incorporating culture-specific norms and practices (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018;), including cultural models of mental health and illness (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018) and incorporating a broader perspective by including religious or spiritual beliefs (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018; Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021). During the implementation of interventions, communication strategies were adapted (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018) with attention to culturally-sensitive language use (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019), socio-cultural barriers and knowledge gaps were addressed through educational approaches (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019), and investments were made in establishing a culture-appropriate (therapeutic) alliance (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021). This was done through the involvement of professionals with either a similar background or the same native language knowledge as the target groups (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019) or professionals being culturally competent or “at least ‘culturally aware’” (Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018). Attention was paid to cultural sensitiveness in therapeutic assignments, examples, and case stories (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019). Some studies adopted a holistic approach to intervention delivery, involving families or a broader social network (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018). Also, (practical) adaptations were made to increase the intervention’s feasibility, such as assuring accessible locations (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021), adjusting the length or timing of the intervention (Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021) or providing economic support (Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019).
Table 5. Strategies for cultural adaptation of existing evidence-based interventions

Participatory approaches
A total of 15 studies described explicitly how they involved members of the target group and communities to enhance the feasibility of the intervention. Based on the descriptions in the articles, the different approaches to community involvement can be situated on a continuum of participatory approaches, ranging from a consultation role to a complete participatory process. We labelled these studies along this continuum: from community-informed (CI) over community-shaped (CS) interventions to community-driven (CD) initiatives (Attygalle, Reference Attygalle2020), see Table 3. Community-informed studies consulted community members in the preparatory phase of intervention (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014), for translation of intervention materials (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013; Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018) or made reference to applying a community-based intervention, but researchers maintained the full control of the intervention study. Community-shaped studies actively involved community members throughout the development or implementation of the intervention. Researchers worked in collaboration with community members to ensure the intervention’s cultural appropriateness. This was done by Gater et al. (Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010) as they developed the group activities in their intervention together with voluntary organisations. In other studies, intervention services were provided by community members, for example, community health workers delivering the intervention (Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010; Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012) or giving education sessions (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008). In the study of Chaudhry et al. (Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009) female Urdu-speaking drivers picked up Pakistani women to ensure that family or community members did not object to the women going out alone with a taxi driver. Baskin et al. (Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021) discuss in their scoping review community-centred interventions, which are either implemented in community settings or in a health setting but delivered by the community members and/or the voluntary sector. In the specific study of Lwembe et al. (Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017), the researcher was part of the intervention as participant observer to evaluate the use of a co-production approach to improve access to psychological therapies.
Community-driven interventions went a step further and ensured community participation from the start of the intervention development process until its evaluation. This is extensively elaborated in the research report by Edge et al. (Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018) who co-developed a cultural adaptation of an existing family intervention in partnership with African-Caribbean service users, their families, community members and healthcare professionals. Using a different approach, Malone et al. (Reference Malone, McGuinness, Cleary, Jefferies, Owens and Kelleher2017) developed, implemented, and evaluated an arts-based community intervention to create awareness of suicidality among Irish Travellers in collaboration with the population group throughout the entire research process. Mantovani et al. (Reference Mantovani, Pizzolati and Gillard2017) used a qualitative participatory approach to pilot an outreach intervention addressing the mental health needs of African and African-Caribbean groups, where faith-based organisations, local public services and community services co-produced the pilot project. De Freitas and Martin (Reference de Freitas and Martin2015) applied the framework of the Participation Chain Model to ensure minority user participation in a mental health advocacy project. In the “community conversation” intervention of Knifton et al. (Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010), health and BME community organisations designed and delivered supportive workshops to explore mental health and stigma.
These studies demonstrated that community-based initiatives were promising approaches, and they were able to document positive changes in their envisaged outcomes as described above (see interventions’ effectiveness).
Barriers and facilitators to intervention uptake
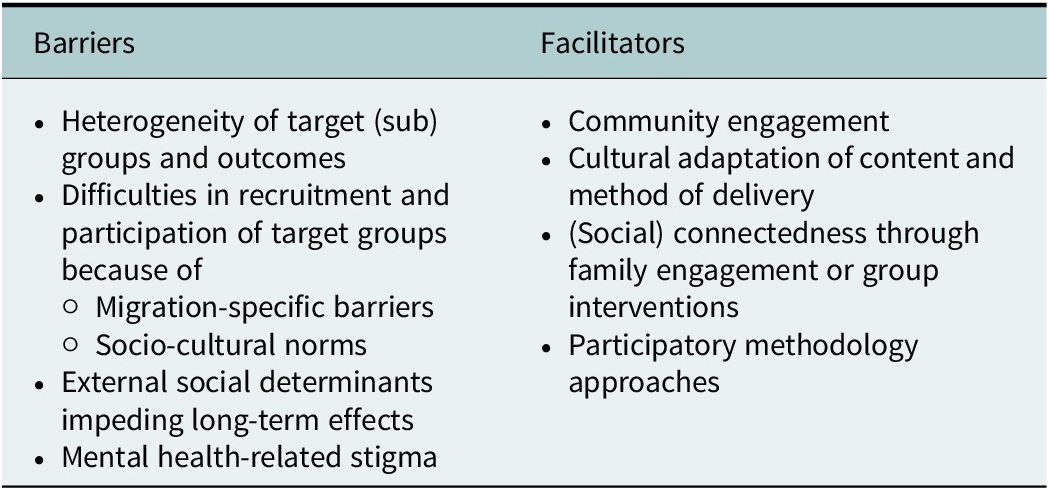
Different barriers impeded the successful implementation of interventions. For instance, the heterogeneity across outcomes and target (sub)groups complicated the cultural adaptation of an intervention (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021). Some authors mentioned that it was difficult to engage the “hard-to-reach” target groups for regular health interventions (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013) and faced poor participation (Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014). According to Lovell et al. (Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014), recruitment to primary care trials in the United Kingdom was generally problematic and especially difficult in mental health trials. The complexities of migration-specific barriers complicate recruitment, as well as the development of culturally acceptable and accessible interventions (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014). The hindering effect of these external, social determinants were often described. Factors such as employment, financial difficulties, legal status, acculturation, racism, and discrimination, might have a large effect on migrants’ and ethnic minorities’ mental health status and therefore might reduce interventions’ (long-term) effects (Osman et al., Reference Osman, Vixner, Flacking, Klingberg-Allvin, Schön and Salari2021). To a similar extent, social problems, many of which are connected to the family context, were brought up by the researchers, especially in those studies describing interventions targeting women. For instance, maltreatment by the husband, problems in raising their children or unavailability of childcare, disabled relatives or divorce were mentioned as impeding interventions’ success (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008; Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019). Due to sociocultural norms, women may experience a lack of autonomy in movement and decision-making, some women expressed that their husband would prevent them from participating in treatment (Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019). The resistance from family members was subject to the stigma on mental health and fear of anticipated disclosure of mental health problems to the “outside” world (Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010). Maintaining family honour and a need to keep up appearances within the community, hinders these target groups from participating and mental health problems are likely to be covered up (Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019). Mental health stigma was experienced as a major barrier among different target groups (Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017; Mantovani et al., Reference Mantovani, Pizzolati and Gillard2017; Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018), but at the same time attempted to be broken down by specific intervention studies, such as by Mantovani et al. (Reference Mantovani, Pizzolati and Gillard2017).
Community engagement emerged as a potential facilitator to engage people from target groups more easily (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014). People felt connected with a provider or with the intervention itself, when they were able to relate to the content of it, felt being listened to, and experienced their needs to be accommodated (Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018; Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021). This provided them with a sense of empowerment (Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018), which might disrupt power balances and may give room to dialogical and equitable encounters (de Freitas and Martin, Reference de Freitas and Martin2015). Making meticulous (cultural) adaptations to the contents and method of delivery to this target group is thus essential (Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003). (Social) connectedness can be facilitated by cultural adaptation of intervention, such as adaptations to language, adaptations in the domains of concepts and illness models, cultural norms and practices, considering explanatory models of illness, incorporating spiritual/religious activities, and acknowledging culture-specific familial structures (Degnan et al., Reference Degnan, Baker, Edge, Nottidge, Noke, Press, Husain, Rathod and Drake2018), inclusion of narratives delivered by community service users (Knifton et al., Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010) or making organisation-specific cultural adaptations (Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021). Another key factor in engaging and retaining participants was engagement with their families (Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019), and also group interventions were evaluated positively in creating this feeling of social connectedness (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014). This connectedness can be further enhanced through participatory approaches, by involving migrant health educators (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008), training lay health workers from the same community to deliver the intervention (Baskin et al., Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021), using expert patients, and giving ownership of intervention modalities or shared decision-making of stakeholders (Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017; Table 6).
Table 6. Barriers to and facilitators for successful intervention uptake
Discussion and conclusions
This scoping review mapped and synthesised studies of interventions designed to improve the mental health or mental well-being of migrants and ethnic minority groups living in Europe. Such interventions are highly needed as these groups are at higher risk for mental health problems than Europe’s general population (Carta et al., Reference Carta, Bernal, Hardoy and Haro-Abad2005; Marmot et al., Reference Marmot, Allen, Goldblatt, Boyce, McNeish, Grady and Geddes2010; Missinne and Bracke, Reference Missinne and Bracke2012). Because of structural inequalities in society (Carta et al., Reference Carta, Bernal, Hardoy and Haro-Abad2005; Missinne and Bracke, Reference Missinne and Bracke2012), stigma associated with mental health (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008), language barriers (Bhui and Bhugra, Reference Bhui and Bhugra2004), and different cultural perceptions of what may constitute mental health problems (i.e., differing explanatory models; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014), tailored approaches and interventions are required to reach these population groups. Our review shows that attention to meet these specific demands is increasing. Yet, given the result of the limited amount of only 27 studies over a period of 22 years, this calls for a greater investment in documenting mental health interventions. Within the selected studies, the effectiveness of some interventions is manifest, while other described interventions were too small-scale or in a pilot phase and need a larger and long-term implementation to evaluate their impact, which impedes us to draw general conclusions on effectiveness and scalability. However, our synthesis and analysis indicate a strong added value of specifically targeting migrants and ethnic minority groups. We identified successful intervention mechanisms to promote mental health in these populations, such as having a sound theory-base, culturally adapting evidence-based interventions, or applying a participatory approach during the development/adaptation of targeted interventions. In what follows, we first critically discuss the findings of our research objectives: (1) the available interventions and their respective outcomes, (2) the intervention mechanisms and cultural adaptation and participatory strategies used, as well as (3) barriers and facilitators for intervention uptake. We then point out the limitations of the selected studies, as well as of our scoping review. Lastly, based on our findings, we map out recommendations for future research, policy, and practice.
Available interventions and outcomes
The findings of this scoping review contribute to an increasing evidence-base of effective mental health interventions. More than half of the studies reported statistically significant results for their envisaged outcomes. If no significant results were found, relevant precursors to improve mental health were identified. Six out of seven randomised trial studies showed positive effects on mental health outcomes, mostly a reduction in depression rates (Jacob et al., Reference Jacob, Bhugra and Mann2002; Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008; Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010; Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019). Also, studies acknowledging the difficulty to conduct RCTs under complex real-life conditions, were able to demonstrate positive effects (e.g., Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012). Furthermore, interventions targeting the social and environmental circumstances in which they were implemented illustrated positive effects. An intervention aimed at changing social relations by improving parent–child interactions positively impacted the mental health of the parents (e.g., Osman et al., Reference Osman, Salari, Klingberg-Allvin, Schön and Flacking2017, Reference Osman, Vixner, Flacking, Klingberg-Allvin, Schön and Salari2021). Lifestyle interventions promoting and facilitating access to physical exercise (e.g., Reijneveld et al., Reference Reijneveld, Westhoff and Hopman-Rock2003; Rabiee et al., Reference Rabiee, Robbins and Khan2015; Siddiqui et al., Reference Siddiqui, Lindblad, Nilsson and Bennet2019) proved to have a positive impact on mental health outcomes. Many smaller and/or qualitative studies indicated promising results or delivered insights into enabling factors for improving mental health and well-being such as improving social functioning (e.g., Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012) or increasing knowledge on mental health conditions (e.g., Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010) or direct support from community members or migrant health educators (e.g., Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010).
Intervention mechanisms, cultural adaptation, and participatory strategies
Not all studies systematically shared information on their assumed intervention mechanisms. Only few studies described systematically, which (set of) changes were effective, how participatory approaches were exactly implemented, or which preconditions were needed to be in place to successfully implement the interventions. We thus cannot identify uniform mechanisms leading to potential effectiveness. However, this review reveals three principles that may increase an intervention’s success: having a sound theory-base, making cultural adaptations, and using participatory approaches. Firstly, our findings show that using a sound theory-base seemed to yield better results (De Silva et al., Reference De Silva, Breuer, Lee, Asher, Chowdhary, Lund and Patel2014). The choice for a specific theoretical underpinning determined the choice for respective interventions strategies or elements, such as using CBT elements (Ünlü Ince et al., Reference Ünlü Ince, Cuijpers, Van’t Hof, Van Ballegooijen, Christensen and Riper2013), peer-support or participatory strategies to increase empowerment (e.g., de Freitas and Martin, Reference de Freitas and Martin2015). Making the underlying theory base explicit, made it easier to assess an intervention’s effect. In addition, it also makes studies replicable, which is an important consideration for further increasing the evidence base. A thorough consideration of an explicit theory of change can contribute to the sustainability of an intervention’s beneficial effects (Mayne, Reference Mayne2020). By grouping the identified intervention mechanisms according to the level of social determinants of health they addressed (see Table 4), we made an effort to fill the gap identified in the literature that current classification systems of mental health interventions do not inherently address health inequities relevant for migrant mental health, such as health disparities based on, for example, ethnic inequities or socio-economic status.
Secondly, cultural adaptations of an intervention increase its acceptability for several reasons. Cultural adaptations enhance the perceived social connectedness among study participants and facilitate access and familiarity with an intervention through the use of cultural reference systems and appropriate language. They contribute to reducing stigma associated with mental health and interventions. Furthermore, culturally adapted interventions consider the specific structural conditions in which many migrants and ethnic minorities live. The level of cultural adaptation among the reviewed studies ranged from translation of materials (Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021), over adapting the content of the intervention by including cultural idioms and metaphors (Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019) to broadening the implementation of the intervention by addressing socio-economic circumstances (Rabiee et al., Reference Rabiee, Robbins and Khan2015). Drawing general conclusions to what extent cultural adaptations should be made and what their nature should be, is challenging given the diversity of the included studies. However, a one-size-fits-all approach may not address the diverse needs of different migrant and ethnic minority populations. However, involving communities affected may help to tailor the needed services.
Thirdly, the evidence presented here shows that community involvement and participatory strategies – preferably starting from the conceptualisation of the (or: adaptation of) the intervention – facilitate its development and successful implementation. Actively involving the communities not only contributes to solely adapting the intervention itself, but also creates cohesion and empowerment among the participants. Studies showed that including patients and their families as well as community leaders can be essential to overcome recruitment barriers and low participation rates (Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014; Dowrick et al., Reference Dowrick, Bower, Chew-Graham, Lovell, Edwards, Lamb, Bristow, Gabbay, Burroughs, Beatty, Waheed, Hann and Gask2016; Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017; Edge and Grey, Reference Edge and Grey2018; Riza et al., Reference Riza, Kalkman, Coritsidis, Koubardas, Vassiliu, Lazarou, Karnaki, Zota, Kantzanou, Psaltopoulou and Linos2020; Baskin et al., Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021). Reasons for reluctance to participate in interventions, such as voluntary nature, stigma, trust issues or lack of appreciation may hinder achieving an intervention’s goals (Apers et al., Reference Apers, Richter, Van Praag and Van Praag2021). The extent to which the interventions described in the selected studies were participatory varied considerably: from community-informed where community members were consulted in a preparatory phase (e.g., Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014), over community-shaped interventions (e.g., Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010), to community-driven participatory approaches as the highest form of involvement towards creating community ownership (e.g., Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018). Studies showed that the use of participatory approaches increased effectiveness as it improved social connectedness, power in local decision-making, and even structural issues such as access to safe and affordable housing (Baskin et al., Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021).
Our findings show that in addition to the above-mentioned principles, it is equally important to address the broader socio-ecological community context. Applying a holistic and intersectoral approach is needed, in particular for people and groups living in precarious socio-economic conditions. (Clinical) interventions or treatments for a general audience (e.g., Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008) have encountered difficulties to address these social determinants. Additionally, financial implications cannot be neglected, calling for free or payable access to health promotion activities. Intervention uptake, however, is facilitated when socioeconomic conditions are taken into account, and social contact and cohesion are enhanced (e.g., Rabiee et al., Reference Rabiee, Robbins and Khan2015).
Facilitators and barriers for intervention uptake
Applying (a combination of) these intervention mechanisms is thus likely to increase the feasibility and acceptability of mental health interventions among the intended target groups. These strategies contribute to overcoming barriers related to the stigma on mental health complaints by incorporating diverse explanatory models in healthcare (e.g., Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017; Mantovani et al., Reference Mantovani, Pizzolati and Gillard2017; Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018) or through the co-production of interventions with migrant and ethnic minority communities (e.g., Lwembe et al., Reference Lwembe, Green, Chigwende, Ojwang and Dennis2017; Edge et al., Reference Edge, Degnan, Cotterill, Berry, Baker, Drake and Abel2018), for instance using artistic approaches (Van De Venter and Buller, Reference Van De Venter and Buller2015; Malone et al., Reference Malone, McGuinness, Cleary, Jefferies, Owens and Kelleher2017). Also, the holistic nature of many mental health complaints, related to the structural living conditions in which ethnic minorities and migrants live, should be considered to a larger extent (e.g., Knifton et al., Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010; Mantovani et al., Reference Mantovani, Pizzolati and Gillard2017). However, hindrances related to these mechanisms should also be acknowledged. Again, the observed heterogeneity of interventions and target groups complicated defining which level of specificity cultural adaptations should have. While interventions often yielded successes in finding coping strategies to deal with mental health problems by introducing direct support from migrant health professionals, it seemed to be far more difficult to increase social support from participants’ direct personal environment (Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008). External, socio-ecological factors, as well as other social problems such as stigma on mental health from the near social environment created resistance to participation. Existing notions on how to engage social networks for all participants were challenged (Chaudhry et al., Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009).
Limitations
Limitations of selected studies
The broad range of described mental health outcomes (e.g., from reducing mental health stigma to reducing suicidal risk) challenges a comparison across studies. While our review identified several examples of pilot and small-scale studies with promising results, many studies were underpowered to assess the envisaged outcomes. These studies should be replicated and evaluated in larger studies using rigorous designs to deliver the needed evidence for upscaling. Additionally, a potential hindrance to scaling up may be the difficulties in the recruitment of participants encountered in several of the intervention studies (e.g., Knifton et al., Reference Knifton, Gervais, Newbigging, Mirza, Quinn, Wilson and Hunkins-Hutchison2010; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014; Van De Venter and Buller, Reference Van De Venter and Buller2015; Christodoulou et al., Reference Christodoulou, Fortune, Arslan and Koc2018). Authors mentioned difficulties in defining and reaching the target groups, and reported poor participation (Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012; Lovell et al., Reference Lovell, Lamb, Gask, Bower, Waheed, Chew-Graham, Lamb, Aseem, Beatty, Burroughs, Clarke, Dowrick, Edwards, Gabbay, Lloyd-Williams and Dowrick2014). This resulted in relatively small sample sizes, short follow-up periods and lack of statistical power. Another review on a similar topic identified transcultural barriers to participation in early intervention research for migrants and ethnic minorities clearly showing a selection bias (e.g., Deriu et al., Reference Deriu, Moro and Benoit2018). The selected studies also did not entail cost-effectiveness measures (with the exception of Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010), yet, cost-effectiveness could be the most convincing argument for policy-makers for scaling-up effective interventions.
The selected articles were also very heterogeneous in terms of the study participants: target groups and inclusion criteria varied across study settings (i.e., specific recruitment criteria), and used different categorisation in different migration and socio-economic contexts. This complicates the comparability of the studies, making it difficult to draw conclusions across studies. Not paying sufficient attention to target-group specific characteristics could also result in overgeneralization (Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021). Additionally, our scoping review revealed a geographic bias. Most studies took place in the United Kingdom followed by the Netherlands and Sweden, and only a few single studies were conducted in other European countries. This bias could be due to differences in investments in the prevention of mental health and addressing underlying health inequalities. For instance, the Equality Act (2010) in the UK might explain the large amount of UK studies, as it has promoted enquiry into ethnic inequalities (Iliffe et al., Reference Iliffe, Walters, Manthorpe, Goodman and Kharicha2017) by explicitly focusing on conducting needs assessments, resource allocation, and health care planning (Acheson, Reference Acheson1998). This has positively impacted research opportunities (Mathur et al., Reference Mathur, Bhaskaran, Chaturvedi, Leon, VanStaa, Grundy and Smeeth2014).
Study limitations
Some limitations of this scoping review should also be pointed out. Due to limited resources, we could not include grey literature, hence we might have missed practice-based evidence often reported by local authorities, civil society organisations and health care practitioners (WHO, 2015). Data extraction was done by single authors, and not in duplicate. In line with the methodology of a scoping review, we did not systematically assess the quality of the included studies, yet we critically reflected on their potential flaws. Furthermore, we opted for interventions in Europe only, however, these regions could also learn from the implementation of interventions outside Europe. Using the categorisation of the public health prevention continuum may also present a limitation. Some studies addressed overlapping stages within the continuum, for example, evidence-based treatment approaches combined with mental health promotion at community level (Eylem et al., Reference Eylem, van Straten, de Wit, Rathod, Bhui and Kerkhof2021; Dubus, Reference Dubus2022). As indicated by Compton and Shim (Reference Compton and Shim2020), this framework does not inherently address health inequities relevant for migrant mental health. To mitigate this, we have synthesised the information available on intervention mechanisms according to the different levels of social health determinants. The broad definition of the population of interest, reflecting the lack of a fine-grained definition, made comparisons across studies difficult. Finally, there may be a bias due to the researchers’ cultural influences and cultural competency indicating the need to develop cultural protocols for researchers and strengthen researchers’ cultural competency.
Recommendations for research and policy
Based on our synthesis, despite the above-described challenges and study limitations, the following recommendations for research and policy can be made.
Research recommendations
First, our scoping review illustrates that evidence on migrant and ethnic minority groups other than refugee and asylum-seekers is scarce and very diverse, few interventions measured the broader social change and reduction in health inequalities and only broadly referred to it in the discussion section. Broadening the scope of research towards other migrant populations would generate more insight into the (common) challenges that these groups face. This could help in addressing the underlying drivers, such as structural issues that affect the mental health of all migrants. Research should invest in studying and addressing the interplay of cultural specificities with socio-ecological factors. Mapping specific mental health outcomes, implemented interventions and outcomes per ethnic minority and migrant group, could work revealingly (Uphoff et al., Reference Uphoff, Robertson, Cabieses, Villalón, Purgato, Churchill and Barbui2020).
Second, our review shows little consistency in defining study populations when considering these “other migrant groups” (e.g., few studies differentiated between first- and second-generation migrants, studies were based on language spoken by participants, studies focussed on “hard-to-reach” migrant groups). To achieve better comparability across studies, future research will therefore benefit from a more streamlined and fine-grained definition of the different categories of migrant population groups, as well as the studies’ geographical location. Studies should clearly specify how migrant and ethnic minority populations are defined, that is, per migration community, legal status, cultural and/or religious background. In doing so, future research could specify per migration community, drivers of migration and cultural similarities with the dominant country. This could further facilitate the understanding of and subsequent narrowing health inequality gaps in different contexts (Lebano et al., Reference Lebano, Hamed, Bradby, Gil-Salmerón, Durá-Ferrandis, Garcés-Ferrer, Azzedine, Riza, Karnaki, Zota and Linos2020; Van Apeldoorn et al., Reference Van Apeldoorn, Agyemang and Moll Van Charante2022).
Third, while stakeholder participation and intersectoral approaches are acknowledged, most interventions remain at the individual level. Participatory interventions, however, not only demand good communication, dealing with linguistic barriers and cultural differences, but also close collaboration of all stakeholders, ranging from governmental actors to ethnic minority and migrant communities (Riza et al., Reference Riza, Kalkman, Coritsidis, Koubardas, Vassiliu, Lazarou, Karnaki, Zota, Kantzanou, Psaltopoulou and Linos2020). There are some promising studies – mostly qualitative accounts of participatory initiatives – to improve mental health outcomes among migrants and ethnic minorities in the EU/EE, but there is a paucity of high-quality evidence regarding these approaches. More studies should look into community-based or community-led approaches.
Fourth, many intervention studies insufficiently considered outcome measures that assess a holistic approach to mental health, and mainly focus on depression or anxiety scales to evaluate interventions. More in-depth analyses on the impact of the different intervention stages could be insightful and yield distinct mental health outcomes as well as the preconditions to successful implementation. In particular, intervention and implementation research would be needed in developing multi-level interventions, addressing both proximal and distal intervention outcomes. From a public health point of view, investments should be made in social and health systems research that addresses the quality of mental health interventions taking into account the sociocultural and socioeconomic contexts and approaches (Haro et al., Reference Haro, Ayuso-mateos, Bitter, Demotes-Mainard, Leboyer, Lewis, Linszen, Maj, McDaid, Meyer-Lindenberg, Robbins, Schumann, Thornicroft, Van Der Feltz-Cornelis, Van Os, Wahlbeck, Wittchen, Wykes, Arango, Bickenbach, Brunn, Cammarata, Chevreul, Evans-Lacko, Finocchiaro, Fiorillo, Forsman, Hazo, Knappe, Kuepper, Luciano, Miret, Obradors-Tarragó, Pagano, Papp and Walker-Tilley2014). Future research should systematically assess the specific preconditions for interventions to be effective and to reach the intended target group, as well as its cost-effectiveness (Afuwape et al., Reference Afuwape, Craig, Harris, Clarke, Flood, Olajide, Cole, Leese, McCrone and Thornicroft2010).
Fifth, given the gender gaps in mental health complaints, a more gender-based approach in interventions are needed, and attention should be paid to how gender intersects with other social determinants of mental health and ethnicity (Bhugra, Reference Bhugra2004; D’Souza and Garcia, Reference D’Souza and Garcia2004; Van De Venter and Buller, Reference Van De Venter and Buller2015; Baskin et al., Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021). Also, given the explicit focus in some studies on women (Jacob et al., Reference Jacob, Bhugra and Mann2002; Kocken et al., Reference Kocken, van Zwanenburg and de Hoop2008; Chaudhry et al., Reference Chaudhry, Waheed, Husain, Bhatti and Creed2009; Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010;Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019), for instance when focusing on post-natal and maternal related mental health (Hesselink et al., Reference Hesselink, van Poppel, van Eijsden, Twisk and van der Wal2012; Khan et al., Reference Khan, Lovell, Lunat, Masood, Shah, Tomenson and Husain2019), or depression (Gater et al., Reference Gater, Waheed, Husain, Tomenson, Aseem and Creed2010), it would also be of added value to focus more on men. Understanding their specific explanatory models on mental health, perceived masculinity, and power dynamics in the household would give insights in potential barriers to mental health services. In turn, this could improve both men’s and women’s participation in interventions on mental health.
Policy recommendations
Some policy recommendations can also be formulated. A holistic approach to mental health, considering the potentially differing explanatory models between healthcare practitioners and ethnic minority groups and migrants, as well as the socio-economic circumstances in which most migrants and ethnic minorities live, needs to be implemented in future interventions and policies. It is important that the social determinants defining ethnic minorities’ and migrants’ vulnerabilities to mental health problems are addressed. However, as we ranked the studies in Table 4 according to the levels of social determinants, we conclude that only few interventions target the resettlement stressors, such as socio-economic and living circumstances, legal residence procedures, detention procedures, and experiences of discrimination and racism (Priebe et al., Reference Priebe, Giacco and El-Nagib2016; Lindert et al., Reference Lindert, Schouler-Ocak, Heinz and Priebe2008; Nosè et al., Reference Nosè, Ballette, Bighelli, Turrini, Purgato, Tol, Priebe and Barbui2017; Von Werthern et al., Reference Von Werthern, Robjant, Chui, Schon, Ottisova, Mason and Katona2018). This might be explained by the fact that structural factors are difficult to change and might require structural policy adaptations, such as an intersectoral health-in-all approach (WHO, 2015). However, addressing the societal context is crucial for prevention strategies, as it is often where the mental health challenges that these groups are confronted with arise (Marsella, Reference Marsella2011). This requires a holistic and interdisciplinary approach, involving governmental actors who have the power to influence harmful structural factors. Hence, policy makers should invest in efforts to streamline services so they fit and interact better together to facilitate the implementation of a holistic approach. Some authors argued (Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021) that culturally adapted care is needed, in which all interventions, services and treatments are suited for different cultural values, patterns, behaviours and beliefs. This could start with a better representation of ethnic diversity within the healthcare systems, as noted by Baskin et al. (Reference Baskin, Zijlstra, McGrath, Lee, Duncan, Oliver, Osborn, Dykxhoorn, Kaner, LaFortune, Walters, Kirkbride and Gnani2021).
Furthermore, needs assessment, tailored health care planning and resource allocation (Acheson, Reference Acheson1998) could be facilitated by the registration of ethnicity, and migration background (Lebano et al., Reference Lebano, Hamed, Bradby, Gil-Salmerón, Durá-Ferrandis, Garcés-Ferrer, Azzedine, Riza, Karnaki, Zota and Linos2020; Van Apeldoorn et al., Reference Van Apeldoorn, Agyemang and Moll Van Charante2022). This way, the needs of local ethnic minority and migrant groups, as well as the specific risks and needs concerning mental health, could be better assessed to make healthcare culturally adapted (Arundell et al., Reference Arundell, Barnett, Buckman, Saunders and Pilling2021), and to foresee some targeted additional interventions oriented at reducing mental health complaints of ethnic minority and migrant groups. Finally, medical interventions, healthcare systems and practices undergo constant transformations, such as digital transformations in communication, assessment, and follow-up. More attention should be paid to a still existing digital divide for migrants and ethnic minorities, which COVID-19 has revealed (Nöstlinger et al., Reference Nöstlinger, Van Landeghem, Vanhamel, Rotsaert, Manirankunda, Ddungu, Reyniers, Katsuva, Vercruyssen, Dielen and Meudec2022). More insights are needed into accessibility, cultural attitudes, and migration-specific experiences of such digital tools (Marwaha and Kvedar, Reference Marwaha and Kvedar2021).
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2023.15.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2023.15.
Data availability statement
All articles are publicly available in the described databases and an appendix of Supplementary Materials is available online.
Acknowledgements
The authors thank the Global Mental Health editors’ team for their assistance throughout the writing and publication process.
Author contribution
C.A. and H.A. defined the scope of the review. H.A., L.V.P., and C.N. determined the review methodology, conducted the review, and wrote a first version of the manuscript, which was revised by C.A. All authors reviewed the final manuscript.
Financial support
The authors received no financial support for the research, authorship, and publication of this article.
Competing interest
The authors declare no conflict of interest with respect to the research, authorship, and publication of this article.
Ethics standard
The protocol of the study has been registered at the Center for Open Science (https://doi.org/10.17605/OSF.IO/R8SBF).










 Open access
Open access
Comments
No accompanying comment.