

Becoming a Feeling and Body Investigator
Welcome! This program will help you support and treat children who experience frequent and impairing abdominal pain. You will help these children trust their bodies and feel safe in them, a mission we accomplish by training everyone (yourself included) to be Feeling and Body Investigators – FBI agents – Pain Division. Through this training, we create an emotional context of exploration and inquisitiveness toward body sensations and provide concrete strategies so that the experience of pain is not scary, but rather a clue, an object of curiosity, and a mystery to be investigated. We treat our strategies as cryptographic tools that help children decipher and respond to the various messages their bodies are communicating, whether these messages are the cramps of hunger pain, the butterflies of anxiety, or the pressure of gas pain.
It may surprise you to think that focusing more on physical sensations can actually reduce the frequency and intensity of pain experiences and improve children’s emotional awareness and regulation. The key to improvement lies in the quality of that attentional focus: it should be one of playful inquiry rather than of anxious hypervigilance. We teach children a new way to interpret their bodies’ physical signals. And perhaps equally important, we foster this same mindset in the parents of these children – both in how they relate to their own bodies and in how they respond to the experiences of their children.
Who can put the FBI program into practice? We have written for a broad audience. Any health professional who works with children in pain, whether in a primary care, school, or therapy setting, can implement this treatment. It should be accessible enough for a trainee but also interesting enough for seasoned clinicians.
By the time you have learned this program, the way in which your practice engages with patients about body symptoms generally and pain specifically will have become a lot more fun as well as more effective. You may even find that your own relationship to your body will have improved. You are officially on the path to becoming a certified Feeling and Body Investigator – Pain Division. Congratulations! We are an elite group of special forces.
How It All Started
The FBI intervention actually arose from my work with an entirely different patient population – children, adolescents, and adults with eating disorders. Amidst numerous other complexities, individuals with eating disorders did not trust the messages their bodies were sending. For example, instead of recognizing a growling stomach as a sign of hunger, they might interpret this discomfort as the body trying to trick them into eating. They saw the emotions and drives of the body as threatening. They treated the body not as an essential life-partner, but as an enemy – something that needed to be subdued, ignored, or punished. This kind of thinking led to life-threatening disorders such as anorexia nervosa; but also, at a more basic psychological level, these individuals did not know themselves – what they wanted, needed, or cared about. Thinking about their experiences led me to wonder how children learn to develop a sense of trust in their body’s wisdom and how to teach this trust when it was not present.
I began to ask myself a lot of very interesting questions. How do children learn to develop a sense of trust and awe at their bodies’ power and wisdom? What type of life experiences could interfere with the emergence of this sense of trust? Could you teach children to trust their bodies when they already had some life experiences that challenged this sense of trust? When do you start? If you do intervene early, can you actually prevent the emergence of psychiatric disorders rooted in distrust of the body? Among many answers to these questions, one theme appeared repeatedly: children with early medical conditions, particularly those resulting in pain, may come to distrust their bodies.
My colleagues and I began to look for a target population of children for whom an intervention might make a difference. Our goal was lofty. If we could (a) take children who were vulnerable to developing feelings of distrust toward their bodies (or perhaps already had) and then (b) help them experience, instead, that their bodies were invincible, and then (c) show them that this invincibility actually arose from the very thing that they thought made them weak – their pain or other prior vulnerability – that could be something very powerful! We wanted to design an intervention that would help vulnerable children (or really any children) to learn to trust deeply in their bodies, to feel safe, and to feel equipped to handle all of life’s challenges.
The FBI program was thus born. Through funding by the National Institutes of Health in the United States, we conducted a clinical trial targeting five- to nine-year-old children with chronic abdominal pain.
Why This Age Group?
Young children are just learning to make sense of their bodies. A developing child must learn how to decipher the various messages that the body sends, to respond to those messages, and to observe the effects of those responses. In turn, these experiences generate data that help to shape future responses. For example, a child senses a pang in their gut, learns to decipher that sensation as hunger, and grabs a small snack.
The presence of chronic or recurrent pain can disrupt this emerging adaptive self-awareness. Children with chronic pain may fail to link uncomfortable body feelings to common, benign sensations, such as hunger or gas. They may begin to avoid or fear a variety of normal body signals. They may even come to fear their bodies.
Our job as FBI agents is to change this trajectory, to alter this framework so that body sensations are viewed with wonder rather than trepidation. As you will see, we take a holistic approach to this awareness: we teach children to recognize all aspects of their experience – not just to develop an awareness of pain and the ability to delineate between types of pain. Children learn to recognize their emotions, to savor sensations like relaxed muscles or a cheery moment, to improve their awareness of basic motivational drives such as hunger, thirst, and fullness, to know what sleepiness feels like and not to become alarmed when Mind-Racing Mikella pays them a visit in bed.
In addition to intervening during a key developmental period, we targeted this age group for another very important reason. We wanted to equip children with tools in body trust so that they were ready for the onslaught of puberty. Think about all the intense, unpredictable, and complicated sensations that erupt as puberty begins. Cramps. Bloating. Surges of anger. Profound waves of sadness. Rejection. Maddening crushes. As puberty starts to unfold, unpredictable hormone fluctuations produce novel body sensations and new levels of emotional intensity (which can also be experienced as intense body sensations). These surges in body intensity may occur at inconvenient and unwanted times – or may be unwanted by their very nature and intensity. Not surprisingly, someone who enters puberty with a deep distrust of their body is going to be very vulnerable. This may set the context for eating disorders, and other psychiatric disorders rooted in fear of the body, to emerge during puberty and early adolescence, their typical age of onset.
Therefore, arming vulnerable children with a profound sense of trust in their bodies seemed like an optimal idea – not only to protect children from experiencing intense sensations as threatening, but also to provide them with a sense of self-awareness that would prepare them for the onslaught of puberty. Imagine what you could accomplish if, at the age of five, you deeply trusted in the power and wisdom of your body and had achieved a sense of profound self-awareness. There would be no stopping you!
Yet, children who are five to nine years old are tough customers. They are not going to stick with a treatment that is not fun, does not make sense, and does not help. We viewed this tough-minded set of consumers as our greatest challenge: if we could satisfy this group, we knew we were onto a winning formula for an intervention strategy. Thus, starting young gives us several critical advantages and keeps us on our toes. We will next touch briefly on our current understanding of recurrent abdominal pain and relate this to the core components of FBI – Pain Division.
Why Children with Abdominal Pain?
Approximately one in ten children or adolescents experience recurrent abdominal pain episodes, episodes of pain that are severe enough to interfere with their daily functioning.Reference Korterink, Diederen and Benninga1 For some, this pain is chronic. For example, children who experienced recurrent abdominal pain at the ages of two, eight, or ten years old were more than twice as likely to have pain at the age of 17.Reference Stein, Pearson and Stein2
Children with pain often avoid activities. For example, 80.5% of children with recurrent abdominal pain missed school during the past quarter relative to 44.6% of children without pain. Chronic absenteeism (missing > 15 days of school) was six times greater in children (6 to 17 years old) with various forms of pain, including abdominal pain, relative to children with no pain,Reference Groenewald, Giles and Palermo3 a consistent finding across studies.Reference Mehta, D’Amico and Luo4 Notably, only 7.2% of children with recurrent abdominal pain participated in six to ten hours of sports per week, relative to 92.8% of children without pain!Reference Devanarayana, de Silva and de Silva5 Child pain is also associated with family-level suffering: parents report reduced healthcare quality of life that they attribute to the emotional consequences and time demands of having a child with recurrent pain.Reference Devanarayana, de Silva and de Silva5,Reference Calvano and Warschburger6
Early pain is also a vulnerability marker for psychopathology. In children who presented to their primary care physician with recurrent abdominal pain, the odds of receiving a current or lifetime anxiety disorder diagnosis were approximately five times greater, and for a lifetime depression diagnosis two times greater when compared to children without a pain presentation.Reference Shelby, Shirkey and Sherman7 Several population-based studies have reported similar findings: the presence of pain in children increases the likelihood for both a concurrent and prospective depression or anxiety diagnosis, in addition to increasing risk for chronic pain.Reference Ayonrinde, Ayonrinde and Adams8
As these findings highlight, it is challenging to parent a child with recurrent pain. Take, for instance, the remarkable discrepancy in sports participation between children with or without pain and consider this particular choice point for parents: deciding whether to enroll your child with recurrent pain in organized team sports. On the one hand, you know the social and emotional benefits of participating in organized sports and have been told by doctors about the benefits of exercise to facilitate pain management.Reference Vierola, Suominen and Lindi9–Reference Kichline, Cushing and Ortega11 On the other hand, given that pain is unpredictable, you do not want your child to get down on themselves or feel that they have let their team down because they are not able to play one day. As a parent, you do not want to risk reneging on your commitments to the team, and you worry that further pressure will actually precipitate more pain episodes. We can all appreciate how difficult navigating these choices can be for parents.
Thus, recurrent abdominal pain is costly to both the individuals experiencing pain and their families. It contributes to the restriction of a child’s activities during key developmental periods when they are learning and practicing skills to improve academic and social competence.Reference Meijer, Sinnema and Bijstra12 It contributes to diminishing feelings of mastery and increases guilt and worry in parents. These studies point to two necessary components for an intervention for recurrent abdominal pain: (1) Start with young children, and (2) Include tools not only to help manage pain, but also to manage intense emotions.
These findings also point to another essential ingredient of an intervention for recurrent abdominal pain: we need to give parents tools so that they feel confident and comfortable with the decisions they make about pain management and related questions, like when to encourage their child to participate in activities such as organized sports.
A Word About Words
In the latest nosology for diagnosing gastrointestinal disorders of gut–brain interaction (also referred to as Functional Gastrointestinal Disorders) published by the Rome Foundation,Reference Drossman, Di Lorenzo and Nurko13 the diagnosis of Functional Abdominal Pain – Not Otherwise Specified is defined by the criteria listed in Table 1.1.
Table 1.1 Functional Abdominal Pain, Not Otherwise SpecifiedReference Drossman, Di Lorenzo and Nurko13
| A child has episodes of abdominal pain at least four times a month. These episodes have a variety of possible triggering or exaggerating events and do not occur solely during eating or other physiological events such as menstruation. While children can be diagnosed with multiple functional gastrointestinal disorders, there is not sufficient criteria for other disorders such as irritable bowel syndrome, functional dyspepsia, or abdominal migraine, or, if present, episodes of pain would be beyond what is expected for those disorders. After a reasonable (i.e., not overwhelming the child and family with unnecessary diagnostic tests, see Chapter 5 in this book), the abdominal pain cannot be fully explained by another medical condition. |
Notes:
Functional Abdominal Pain – Not Otherwise Specified (NOS) falls into the class of Functional Abdominal Pain Disorders within the Rome IV Pediatric Functional Gastrointestinal Disorders, Disorders of Gut-Brain Interaction, classification guidelines, first edition, 2016 with guest editors Carlo Di Lorenzo and Samuel Nurko and the Rome IV Pediatric Committee. Dr. Douglas Drossman (senior editor), Lin Chang, John Kellow, William D. Chey, Jan Tack, and William E. Whitehead are the editors of the series. For the clinical trial of FBI – Pain Division, we screened children directly from primary care. They had to meet the Rome III criteria for Functional Abdominal Pain in terms of pain frequency or intensity (e.g., weekly pain or a particularly impairing pain episode over the past month), but we were liberal in the presence of other abdominal, pain-related functional gastrointestinal disorder (AP-FGID). We reasoned that the strategies employed in FBI – Pain Division would be applicable across the spectrum of abdominal pain predominant functional GI disorders. The name Functional Abdominal Pain, Not Otherwise Specified is new to the Rome IV classification and is meant to help with greater specificity of diagnosis for research purposes. For the purpose of this guide, we use the term Recurrent Abdominal Pain to reflect this broad inclusion of pain-related functional gastrointestinal disorders.
It is notable that the use of the term functional has a rather complicated history and was used to refer to gastrointestinal disorders that were related to problems in function, rather than structure. However, an unfortunate connotation of this definition is that the etiology of functional pain disorders is behavioral or psychological rather than biological (i.e., individuals’ descriptions of pain have a “function” – to avoid an unwanted activity, to get attention, etc.), a formulation that is increasingly outdated given researchers’ and clinicians’ increasingly refined understanding of the complex, influential, and constant reciprocal interactions of the gut–brain axis.Reference Drossman14
As our conceptualization of these disorders has gotten more nuanced (see the next section), the term functional is still employed, more for historical reasons, and disorders of gut–brain interaction is a term that is thought to better reflect the complex etiology and maintenance of these disorders.
To bypass this complexity in nosology, we will use the term recurrent abdominal pain (RAP) throughout the remainder of this book to refer to children who have recurrent episodes of abdominal pain that impair functioning. That said, the strategy of this intervention, with its focus on body awareness and body curiosity, would arguably be appropriate to aid in the management of the class of pain-predominant pediatric functional gastrointestinal disorders classified in the ROME IV classification system.Reference Hyams, Di Lorenzo and Saps15
Approach To This Book
This book is divided into three sections. Part I reviews the scientific background that supports our intervention strategy. This material will help you understand the fundamental principles that guide the intervention so that you can be flexible in its application – not bound to a rigid script or set of techniques performed in prescribed ways. Part II presents the intervention, walking you through each session and its components, translating the scientific principles into suggestions of implementation strategies. If you are eager to get started, you could skip to Part II and begin the treatment. Then, when you are curious about why it is working, you can go back and read Part I to enhance the meaning of your observations as an FBI provider. Just as there is no one right way to implement this intervention (the implementation itself is also in the spirit of investigation), such may be your attitude toward this book: there is no one right way to read it. Finally, Part III provides you with handouts, workbook pages, resources for additional trainings, web-based family communities your patients may join, and therapist communities you may access to augment your treatment delivery.
Throughout, when referring to singular individuals, we will include the use of the pronouns they/them to be as inclusive as possible.
We hope you enjoy reading this book as much as you will enjoy conducting the FBI – Pain Division intervention.
Conceptualizing Disorders of the Gut–Brain Axis
There has been a transformative reconceptualization in the way in which a particular class of gastrointestinal disorders, functional gastrointestinal disorders, are understood. Disorders such as functional abdominal pain – not otherwise specified are understood to arise in vulnerable individuals. What makes an individual vulnerable differs, but vulnerability can arise from a complex interplay of early life experiences that sensitize the gut–brain axis to pain, from genetic contributions, and/or from environmental stressors including those experienced as traumatic. For example, Thapar et al.Reference Thapar, Benninga and Crowell16 describes a model of sensitizing medical events, sensitizing psychosocial events, and genetic predispositions that increase the vulnerability of the microbiota gut–brain axis (see Thapar et al.Reference Thapar, Benninga and Crowell16 for a review). Upon this vulnerable backdrop unfolds complex interactions between bottom-up influences related to gut physiology and top-down influences from the central nervous system that both influence and are influenced by input from the gut (Figure 1.1). In other words, interacting influences from the central nervous system (e.g., vigilance and attention directed toward detecting symptoms, fear about body sensations, perceived stress); sensory systems (e.g., individual differences in the intensity of sensory signaling, capacities to notice changing visceral sensations and the experienced intensity of those sensations – a construct known as visceral hypersensitivity); the gut environment (e.g., the communities of gut bacterial flora composition that influence host health); and the body’s defensive responses against disease or perceived somatic threats (e.g., immune responses, inflammation) all interact to influence the symptoms and severity of functional GI disorders – i.e., disorders of gut–brain interaction. One theme that emerges from this conceptualization of disorders of the gut–brain axis is that no process occurs in isolation, but, of course, is part of a dynamic system.
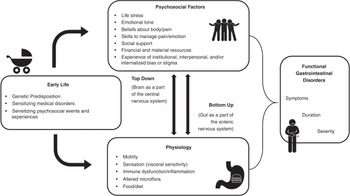
Figure 1.1 This figure is by no means meant to provide a comprehensive listing of all the factors that influence gastrointestinal symptom onset and maintenance. Rather, the central messages of this figure are that various categories of influences (e.g., psychosocial, physiological,) are reciprocal in influence – each impacting the other, while early developmental factors may increase vulnerability to the potentiation of these processes. This conceptualization actually offers hope regarding clinical intervention: addressing any part of the model may impact multiple facets. However, this model also presents challenges: how do we choose one intervention powerful enough to influence other factors? Furthermore, we must recognize that some aspects of the model may be more modifiable than others
The first impression one may gather from looking at Figure 1.1 is that disorders of gut–brain interaction are complicated. On the one hand, one can appreciate that this model is a beautiful reflection of an individual’s unique journey across development, one that is embedded within a social and emotional context that impacts physiology which, in turn, influences that context. Yet, as intervention developers, at first glance such models can be a tad overwhelming. Where does one begin to influence change? How does one take into account all of these interlocking and mutually reinforcing factors? Where do we start?
This is where FBI – Pain Division comes in. Here we briefly outline our intervention and show how it interfaces with key nodes of this model to effect change. An important assumption in our approach is that you do not have to target all elements of a system simultaneously; you just have to pick some key nodes, nodes in the system that are powerful enough to have clinically meaningful downstream effects. In Figure 1.2 we highlight how elements of FBI address what we view as key nodes in the system.
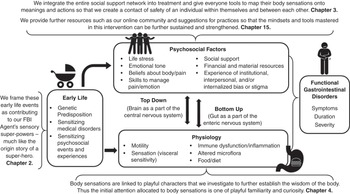
An alternative, and complementary, manner to approach the biopsychosocial model is the attempt to alter the entire backdrop on which this model is unfolding. Figure 1.3 illustrates how FBI – Pain Division also attempts this approach. By creating a context of humor and a mindset that a child’s body is wicked smart and capable of adapting and learning from the most painful and distressing of circumstances, we hope to influence not only events as they unfold in the current moment, but also how one’s history is viewed and how one’s future is regarded. Rather than walk you through each of these components right now, we will gradually work you through them as we go through these chapters.
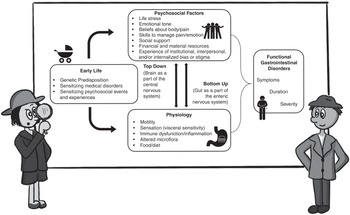
Figure 1.3 Curious FBI agents probe the gut–brain axis. Another way of conceptualizing the FBI intervention is that we are changing the context or backdrop on which disorders of gut–brain interaction operate: all these complex pathways unfold against a backdrop of discerning, investigative wonderment.
The Logic and Core Components of FBI – Pain Division
We believe that children with recurrent abdominal pain have “sensory superpowers.” They notice changes in their bodies that other children do not notice and feel sensations in their bodies with unusual intensity. The technical term for these “superpowers” is “visceral hypersensitivity,” i.e., having low thresholds for noticing and experiencing pain from the viscera and for experiencing other changing visceral sensations. These sensory superpowers may also extend to the external world, in that these children may notice things that other children may not notice and may be deeply affected by the events and emotions of the world around them; these children are little emotional sponges.
Through the FBI program we re-interpret these sensory superpowers as a gift: children with sensitive superpowers live life out loud! They have vivid lived experiences. Their deep and intense feelings make them – quite literally – sensitive children who can make the world a better place in which to live. FBI – Pain Division teaches these children how to harness these superpowers so that they enrich their lives rather than get in the way.
Table 1.2 summarizes the core components of the FBI – Pain Division intervention.

Each weekly session consists of several consistent elements – Body Sensations, Body Investigations, Body Map, Body Brainstorms, and Body Clues – while focusing on the introduction of a new theme (e.g., eating and drinking, high-energy negative emotions, low-energy negative emotions, high-energy positive emotions, digesting food, sleeping, relaxing) and silly characters related to that theme (see Table 1.2). For example, the Groovies and Shakies, Part 1, are sensations related to high-energy negative emotions, whereas the Blahs are the category for low-energy negative emotions.
The Body Sensations characters represent distinct body sensations (e.g., Gassy Gus, Patricia the Poop Pain, Georgia the Gut Growler). Each playful cartoon illustrated in the workbook (Part 3) teaches the meaning of a bodily sensation.
Body Investigations are conducted every session to learn new things about how the body handles certain situations. We will learn much more about the art and logic of these investigations in Chapter 4, but for now, know that these body investigations are designed to teach children a lesson about their bodies and help strengthen a mindset in these children that their bodies are strong, capable, and wicked smart.
Each week the forensic team (child, parent, and therapist) summarize all that they have learned on a Body Map unique to that child, much as a detective would organize clues on a crime map.
Body Brainstorms help children generalize what was learned in a treatment session to the world around them. Body Brainstorms guide them to think about other situations in which they have experienced the same body sensations that were the focus of the session.
Finally, as the intervention progresses, children and parents are trained in our Body Clues worksheet. This worksheet helps children link sensations to meanings and then to take whatever action is needed to meet the need communicated by that sensation. For those of you who are well-versed in cognitive behavioral approaches for pain management, a key differentiator of FBI – Pain Division is the focus here on sensations rather than on thoughts to guide monitoring and to increase self-awareness. All these activities are facilitated by therapists and parents who also embody the spirit of inquisitive and playful investigators, a topic we spend time delving into in Chapter 3 and throughout the intervention.
The first three sessions of the workbook and the corresponding worksheets with these sessions are found in Part III of this handbook in black and white. The entire color workbook and color worksheets are available via download from links found throughout the book, because we thought this was the easiest way to deliver the materials. In the clinical trial, we gave parents the workbook pages session by session – mainly because the children got so excited to learn the new characters in a big “reveal” each week.
Before we leave this chapter, let’s revisit the dilemma of a parent who is deciding whether to enroll their child with recurrent abdominal pain in an organized sports program. Since we last visited this family, they have been trained as official FBI Agents – Pain Division. Armed with the spirit of adventure, the parent decides that they will enroll their child in baseball. When an episode of pain occurs on the day of a practice or game, parent and child will design a series of investigations that they are going to explore. Here are a few examples:
If I think I’m feeling Gassy Gus, can I swing the bat hard enough or run fast enough that it makes me fart?
What happens to the pain when I run? Does it stay in the same place? Move around? If it does move around, can I do a couple experiments where I try to see where I can move it exactly where I want it?
If I do fart when I run, does that make me run faster? Like the gas from the fart is propelling me onward?
When they get home, they will add what they have learned to their Body Map. As it turns out, the child decided they needed a new character to capture the bouncing nature of the pain as they ran. And thus, Bouncy Bart Butt was born.
And that is an example of one part of the science and “elegance” of FBI – Pain Division.
Let’s start our first mission.





