


The proportion of elderly individuals in the population of industrialised countries is steadily increasing. This increased longevity has been mainly attributed to environmental factors such as improvement in medical care, better living standards and improved nutrition. In recent decades, a large amount of information has been accumulated about the possible widespread occurrence of Zn deficiency (Brown et al. Reference Brown, Wuehler and Peerson2001; Maret & Sandstead, Reference Maret and Sandstead2006) in ageing and the various associated health consequences for the elderly such as reduced immunocompetence (Mocchegiani et al. Reference Mocchegiani, Muzzioli and Giacconi2000; Moroni et al. Reference Moroni, Di Paolo, Rigo, Cipriano, Giacconi, Recchioni, Marcheselli, Malavolta and Mocchegiani2005), osteoporosis (Cashman & Flynn, Reference Cashman and Flynn1998; Hyun et al. Reference Hyun, Barrett-Connor and Milne2004), oxidative stress (Junqueira et al. Reference Junqueira, Barros, Chan, Rodrigues, Giavarotti, Abud and Deucher2004), and diabetes (Strain, Reference Strain1991; Singh et al. Reference Singh, Niaz, Rastogi, Bajaj, Gaoli and Shoumin1998). Long-term marginal intakes of Zn coupled with a decreased absorptive efficiency could severely compromise Zn status in older individuals. This suboptimal status might be responsible for the high incidence of alteration of the immune system and degenerative pathologies related to age (Ekmekcioglu, Reference Ekmekcioglu2001; Meunier et al. Reference Meunier, O'Connor, Maiani, Cashman, Secker, Ferry, Roussel and Coudray2005). Thus, Zn supplementation may afford a benefit to ameliorate these age-related pathologies. Several studies using nutritional doses or supra-nutritional doses of Zn have shown interesting results in institutionalised or hospitalised subjects on immunity (Peretz et al. Reference Peretz, Neve, Jeghers and Pelen1993; Fortes et al. Reference Fortes, Forastiere and Agabiti1998; Girodon et al. Reference Girodon, Galan, Monget, Boutron-Ruault, Brunet-Lecomte, Preziosi, Arnaud, Manuguerra and Herchberg1999). However, data on the effect of Zn supplementation in healthy free-living elderly are scarce. Furthermore, the use of Zn supplements in the free living is still a matter of debate as supplemental Zn doses greater than the European RDA of 15 mg (Commission of the European Communities, 1993) over several months have been reported to be associated with impairment of the immune response (Chandra, Reference Chandra1984; Dardenne, Reference Dardenne2003), adverse effects by decreasing Cu and Fe bioavailability (Disilvestro & Cousins, Reference Disilvestro and Cousins1983; Solomons, Reference Solomons1986; O'Brien et al. Reference O'Brien, Zavaleta, Caulfield, Wen and Abrams2000), and a decline in serum HDL (Hooper et al. Reference Hooper, Visconti, Garry and Johnson1980; Black et al. Reference Black, Medeiros, Brunett and Welke1988). The balance among micronutrients within the body appears to be finely regulated and it is, therefore, very important, particularly among the elderly, for whom deficiency in one or several micronutrients may have functional consequences for health. Zn supplementation, at pharmacological (160 to 300 mg/d) or supra-nutritional (30 to 60 mg/d) doses resulted in lower HDL-cholesterol in healthy adults (Hooper et al. Reference Hooper, Visconti, Garry and Johnson1980), which may be related to the negative effects on Cu status (He et al. Reference He, Tell, Tang, Mo and He1992). Results from those studies were not conclusive but raised important public health issues. Assessing the effect of a single Zn supplementation on the biochemical indicators of Fe and Cu status could help to determine whether adverse effects are associated with Zn supplementation at one to two times the RDA. It was, therefore, important to critically evaluate the possible beneficial or adverse effects of Zn supplementation of intakes in the elderly through a randomised, double-blind, placebo-controlled intervention trial of Zn supplementation, with higher doses than the RDA.
The overall objective of the Zenith Project was to investigate the potential of Zn given as a nutritional supplement to late middle-aged and older free-living European population, in order to establish beneficial effects on psychological and behavioural factors and on surrogate markers (oxidative stress, immunity, thyroid function, bone metabolism and protein synthesis).
The objectives of the present study as a part of the Zenith Project were to measure the efficiency of Zn supplementation at nutritional and supra-nutritional doses on Zn status according to age, sex and duration of supplementation: (a) to increase Zn status in the elderly and (b) to evaluate the safety effects of Zn supplementation on the status of trace elements absorbed competitively with Zn (Cu, Fe), and on lipid profile in Zn-supplemented free-living apparently healthy elderly individuals.
Subjects and methods
Design
A total of 387 volunteers participated in the large multi-centred European Zenith Study. Subjects (n 188) aged 55–70 years (61·8 ± 4·4 years), recruited from Clermont-Ferrand (France) (n 95) and Coleraine (UK) (n 93), constituted the late middle-aged group, and 199 subjects aged 70–85 years (74·4 ± 3·8 years), recruited from Grenoble (France) (n 91) and Rome (Italy) (n 108), constituted the older group. Details of subject recruitment and screening, including inclusion and exclusion criteria, as well as of ethical considerations have been described in a previous article (Polito et al. Reference Polito, Intorre and Andriollo-Sanchez2005a, Reference Polito, Meunier and Andriollo-Sanchezb). Briefly, volunteers were invited to attend a preliminary session that included a full medical history and examination, undertaken by a medical doctor, including anthropometric measurements, and screening for cognitive impairment by the Mini-Mental State Examination (Folstein et al. Reference Folstein, Folstein and McHugh1975) and depression (Geriatric Depression Scale; Yesavage et al. Reference Yesavage, Brink, Rose, Lum, Huang, Adey and Leirer1983). Dietary habits were evaluated with a FFQ (SU.VI.MAX, 1994; DietroMetro, 1999). Fully informed written consent was required before taking part in the study. Ethical approval was obtained from the appropriate ethics committee in each of the three countries involved in the study. Exclusion criteria were as follows: smoking more than 10 g tobacco/d; alcohol consumption more than 30 g alcohol/d for men and more than 20 g/d for women (World Health Organization, 1998; James, Reference James2001); more than three drugs per d for 55–70 years and more than four drugs per d for 70–85 years; medical treatment which might affect Zn status (antidepressant drugs, laxatives or hormone-replacement therapy); pathological diseases (diabetes, hypertension, cancer); taking supplements; a BMI < 20 kg/m2 and >30 kg/m2; a cognitive impairment (Mini-Mental State Examination score) < 23 or depression (Geriatric Depression Scale score) >6.
For participants satisfying the inclusion criteria, a biochemistry profile was performed, which included a full blood profile, and tests of kidney and liver function. On the basis of these data, volunteers were excluded if there was renal insufficiency and hepatic diseases, malabsorption or inflammatory chronic pathologies, and if they presented positive serology for HIV and hepatitis C viruses.
Subjects in each centre were randomised into three groups to receive a matching placebo, 15 mg Zn/d, or 30 mg Zn/d for 6 months. During the 6-month supplementation period each subject took, in addition to their usual diet (with self-selected Zn intake of about 10·5 mg/d), either 15 or 30 mg supplemental Zn/d. The supplemental Zn was given as zinc gluconate, which was prepared and supplied by E-Pharma (Creapharm, Gannat, France). The placebo capsule contained 199 mg lactose and 1 mg magnesium stearate. The 7·5 mg Zn capsule contained 56·9 mg zinc gluconate, 142·1 mg lactose and 1 mg magnesium stearate, whereas the 15 mg Zn capsule contained 113·7 mg zinc gluconate, 85·3 mg lactose and 1 mg magnesium stearate. The capsules of the three batches were identical in their shape, colour and weight. Subjects in the 15 mg Zn group received two 7·5 mg capsules per d and the 30 mg Zn group received two 15 mg capsules daily. The larger dose was determined on the basis of an average adult intake of 10 mg Zn/d and a tolerable upper intake level for adults of 40 mg Zn/d according to WHO (World Health Organization, 1996). Zn capsules were distributed to the subjects at the beginning of the trial and at 3 months. At 3 and 6 months, the subjects were asked to return any remaining capsules, and the degree of apparent compliance was estimated from the number of delivered capsules and the number of returned capsules. Compliance, expressed as a proportion of the intended supplements consumed during Zn supplementation, did not differ among the three groups; the mean compliance was ≥ 98·0 % in all groups. Between 07.00 and 09.00 hours on the last day of each treatment period and during the week immediately preceding the trial (baseline), subjects were instructed to collect fasting first-void urine samples and, after an overnight fast, blood samples were taken.
Ethical considerations
Ethical approval was obtained by all four research centres from the respective ethical committees (see Polito et al. Reference Polito, Intorre and Andriollo-Sanchez2005a, Reference Polito, Meunier and Andriollo-Sanchezb). Before participation in the study, all subjects signed an informed consent document approved by these respective ethical committees.
Dietary intake estimation
At the beginning and at the end of each supplementation period, dietary intakes of micronutrients were estimated using 4 d food-intake record (including weekends). Each volunteer had received a notebook with one record to be completed per meal or snack to fill in. They were required to note for each meal or snack, the names and brand of foods and drinks, and the quantities ingested by an estimation using domestic measurements. The dietary data were checked with a dietitian, and foods quantities were estimated using an instruction manual containing photographs for portions sizes (Le Moullec et al. Reference Le Moullec, Deheeger and Preziosi1996). Food consumption data were converted into energy, and macro- and micronutrients by the relevant food composition tables (Polito et al. Reference Polito, Intorre and Andriollo-Sanchez2005a, Reference Polito, Meunier and Andriollo-Sanchezb).
Laboratory analyses
Collection and preparation of samples
All blood samples (40 ml) were collected after a 12 h overnight fast between 07.00 and 09.00 hours. For trace element determination, blood was sampled into trace element-free tubes specific for trace element analysis (Li-Heparin dark blue vacutainer® tubes; Beckton-Dickinson, Pont de Claix, France). Subjects were supplied with suitable collection containers for urine samples and instructed to collect morning void urine samples. Samples of urine were stored at − 20°C from the morning of collection until required for analysis. To avoid environmental contamination with trace elements, tips of pipettes and vials and any other containers used for preparations of serum and urine samples were previously treated with nitric acid and checked for trace-element contamination. Samples were kept on ice immediately after drawing, and then centrifuged at 1000 g for 15 min at 4°C. Serum, plasma and erythrocytes were immediately isolated, sampled and stored at − 80°C.
To insure high reliability of results, the whole initial and final biological samples for a given biochemical parameter were analysed by the same laboratory.
Zinc status
Serum, erythrocyte and urinary Zn levels were determined by flame atomic absorption spectrometry using a previously described method (Arnaud et al. Reference Arnaud, Bellanger, Bienvenu, Chappuis and Favier1986). Seronorm® trace element serum was used as an internal quality control (Sero®, Billingstad, Norway). Serum alkaline phosphatase activity was determined by photometric analysis with commercially available kits on a Hitachi 912 Clinical Chemistry Auto-analyser (Roche Diagnosis Ltd, Welwyn Garden City, Herts, UK).
Copper status
Serum Cu levels were determined by inductively coupled plasma MS using a Thermo Electron X Series instrument (Thermo Electron, Hemel Hempstead, Herts, UK). Erythrocyte Cu,Zn-superoxide dismutase (SOD) activity was determined on an automatic analyser using a commercially available kit (Randox, Crumlin, Co. Antrim, UK). Measurement of Cu,Zn-SOD enzyme activity was based on the generation of superoxide radicals by xanthine and xanthine oxidase, which reacts with 2-(4-iodophenyl)-3-(4-nitrophenol)-5-phenyltetrazolium chloride (INT) to form red formazan dye (McCord & Fridovich, Reference McCord and Fridovich1969). The Cu,Zn-SOD activity was expressed as U/g Hb. One unit of Cu,Zn-SOD was defined as the amounts of enzyme necessary to produce 50 % inhibition in the INT reduction rate.
Iron status
Hb level was measured immediately by the cyanmethaemoglobin method (van Kampen & Ziljstra, Reference van Kampen and Ziljstra1961). Serum Fe was determined by colorimetric assay. Under acidic conditions, Fe is liberated from transferrin. Ascorbate reduces the released Fe3+ ions to Fe2+ ions, which then react with FerroZine to form a coloured complex. The colour intensity is directly proportional to the Fe level and was measured photometrically. Serum ferritin and transferrin levels were measured using automatic immunoprecipitation on a BN II nephelometer (Dade-Behring, Marburg, Germany).
Urinary creatinine
Creatinine was determined in urine samples using a diagnostic kit (MetraTM Creatinine Assay Kit, catalogue no. 8009; Quidel Corporation, San Diego, CA, USA).
Lipids parameters
Serum TAG, total cholesterol, and LDL- and HDL-cholesterol were measured by automated methods using commercially available kits by photometric analysis on a Hitachi 912 auto-analyser. Commercially available kits were purchased from Roche Diagnostics Ltd.
Statistical analyses
Data are presented as means and standard deviations and were tested by two- or three-way ANOVA using the general linear models procedure of the Super ANOVA package (Abacus, Berkeley, CA, USA). ANOVA assumes that the data are sampled from a population that follows Gaussian distributions. This assumption was tested using the method of Kolmogorov and Smirnov. When the Kolmogorov–Smirnov test suggested that the data distribution does not follow the normal law (erythrocyte Zn, serum alkaline phosphatase, Zn urinary excretion, serum Cu, serum ferritin, erythrocyte SOD, all serum lipid parameters), the data of these parameters were log transformed before statistical analysis. Post hoc comparisons were performed using Fisher's least significant difference procedures. When there was an interaction between the studied factors for a given parameter, the Fisher post hoc test was done testing separately the difference in the response to Zn supplementation within each considered factor (period, age, sex). Differences of P < 0·05 were considered statistically significant.
Results
Subject characteristics and dietary intakes before and after zinc supplementation
Age, BMI and dietary intakes of studied subjects before and after Zn supplementation are shown in Table 1. These parameters were not significantly altered by Zn supplementation. These results show that BMI, energy intake and Fe intake were lower in older subjects than in middle-aged subjects. On the contrary, Cu intake was higher in older subjects than in middle-aged subjects, whereas Zn intake was not statistically different between these age brackets. As expected, all these parameters were lower in women than in men.
Table 1 Age and body mass index of the subjects and dietary intakes at the beginning and at the end of the zinc supplementation trial (Mean values and standard deviations)

Overall effects of zinc supplementation on all subjects
The overall effects of Zn supplementations on trace element status and serum lipid profiles according to Zn doses are shown in Table 2. Serum Zn level, erythrocyte Cu,Zn-SOD activity and urine Zn excretion significantly increased with increasing Zn doses in a time-dependent manner. The other measured parameters (erythrocyte Zn, alkaline phosphatase, Hb, Fe, ferritin, transferrin saturation, Cu and lipid parameters) were not altered by Zn supplementation, although a time effect on blood Hb and serum Fe was observed.
Table 2 Overall effects of zinc supplementation on trace element status and lipid metabolism in middle-aged and older-aged subjects according to administered zinc doses and length of supplementation (Mean values and standard deviations)
ALP, alkaline phosphatase; SOD, superoxide dismutase.
a,b,c Means of a parameter for a given period (baseline, or month 3 or month 6) with unlike superscript letters were significantly different (P < 0·05).
Effects of zinc supplementation according to subject age
As shown in Table 3, serum Zn level and Zn urinary excretion were higher in the older subjects than in the middle-aged subjects (P = 0·012 and P < 0·0001, respectively), whereas erythrocyte Zn level was lower in the older subjects than in the middle-aged subjects (P < 0·0001) and serum phosphatase alkaline was similar in both groups. Serum Fe and blood Hb levels were lower in the older subjects than in the middle-aged subjects (P < 0·0001 and P = 0·020, respectively), whereas serum ferritin level was higher in the older subjects than in the middle-aged subjects (P = 0·0002) and serum transferrin saturation was similar in both groups. Serum Cu level was similar in both groups, whereas erythrocyte Cu,Zn-SOD activity was lower in the older subjects than in the middle-aged subjects (P < 0·0001). As expected, serum TAG, total cholesterol and LDL-cholesterol were higher in the older subjects than in the middle-aged subjects (P < 0·0001), whereas serum HDL-cholesterol was slightly lower in the older subjects than in the middle-aged subjects (P = 0·051) and thus the LDL:HDL ratio was higher in the older subjects than in the middle-aged subjects (P < 0·0001).
Table 3 Overall effects of zinc supplementation on trace element status in middle-aged and older-aged subjects according to subject age (Mean values and standard deviations)

ALP, serum alkaline phosphatase; SOD, superoxide dismutase.
a,b,c Means of a parameter for a given age group (55–70 or >70 years) with unlike superscript letters were significantly different (P < 0·05).
Some of the responses of trace element status and lipid metabolism to Zn supplementation were age-dependent. The response of serum Zn to Zn supplementation was similar in both groups; however, erythrocyte Zn level only increased in the older subjects and not in the middle-aged subjects (P = 0·004). Zn urinary excretion was elevated only in the older subject cohort and not in the middle-aged subject group (P = 0·009). No overall effects on serum alkaline phosphatase with Zn supplementation was seen; however, serum alkaline phosphatase increased in middle-aged subjects receiving 30 mg Zn/d and decreased in older subjects receiving 30 mg Zn/d. Serum Fe, serum Cu, erythrocyte SOD and lipid metabolism responded similarly to Zn supplementation in both age groups (NS). In middle-aged subjects, serum ferritin, transferrin saturation, cholesterol and LDL-cholesterol were increased in subjects receiving 30 mg Zn/d. In older subjects, blood Hb decreased in subjects receiving 30 mg Zn/d.
Effects of zinc supplementation according to subject sex
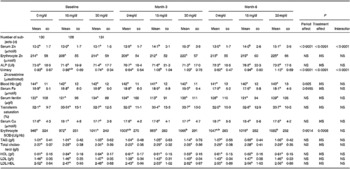
As shown in Table 4, serum alkaline phosphatase and urinary Zn excretion were higher in women than in men (P = 0·010 and P = 0·013, respectively), whereas serum Zn and erythrocyte Zn levels were similar in both groups. As expected, all Fe status parameters (blood Hb, serum Fe and ferritin levels and percentage transferrin saturation) were lower in women than in men (P < 0·0001). Serum Cu level was higher in women than in men (P < 0·0001), whereas erythrocyte Cu,Zn-SOD activity was similar in both groups. Serum total cholesterol, LDL-cholesterol and HDL-cholesterol were higher in women than in men (P < 0·0001, P < 0·0001, P = 0·047, respectively), whereas serum TAG level was lower in women than in men (P = 0·0003).
Table 4 Overall effects of zinc supplementation on trace element status in middle-aged and older-aged subjects according to subject sex (Mean values and standard deviations)

ALP, serum alkaline phosphatase; SOD, superoxide dismutase.
a,b,c Means of a parameter for a given sex group (women or men) with unlike superscript letters were significantly different (P < 0·05).
Some of the responses of trace element status and lipid metabolism to Zn supplementation were sex-dependent. Serum Zn level increased similarly in both sexes, whereas erythrocyte Zn level increased in men but not in women (P = 0·003), and Zn urinary excretion increased only in women but not in men (P = 0·009). Similarly, serum Fe level was increased in women at the dose of 30 mg Zn/d but tended to decrease in men (P = 0·031). The other measured parameters (serum alkaline phosphatase, blood Hb, ferritin, transferrin saturation, serum Cu, erythrocyte SOD and lipid parameters) responded similarly to Zn supplementation in both sexes (NS). Some other significant differences were also observed in the female or in the male group in response to Zn supplementation. In women but not in men, blood Hb decreased whereas serum Fe, ferritin, transferrin saturation and serum TAG level increased after Zn supplementation.
Discussion
There is growing interest in the maintenance of optimal trace element status in ageing; Zn may exert a number of indirect antioxidant functions, suggesting that it may have a preventive role in some diseases associated with ageing (Strain, Reference Strain1991; Singh et al. Reference Singh, Niaz, Rastogi, Bajaj, Gaoli and Shoumin1998; Mocchegiani et al. Reference Mocchegiani, Muzzioli and Giacconi2000; Hyun et al. Reference Hyun, Barrett-Connor and Milne2004; Junqueira et al. Reference Junqueira, Barros, Chan, Rodrigues, Giavarotti, Abud and Deucher2004; Moroni et al. Reference Moroni, Di Paolo, Rigo, Cipriano, Giacconi, Recchioni, Marcheselli, Malavolta and Mocchegiani2005). However, data on Zn supplementation of healthy free-living individuals are scarce and possible adverse effects of a high Zn dose, as suggested in some studies, cannot be ruled out (Chandra, Reference Chandra1984; Chevalier et al. Reference Chevalier, Liepa, Murphy, Suneson, Vanbeber, Gorman and Cochran2002). The aim of the present study was to investigate the effects of Zn supplementation at nutritional (15 mg/d) or supra-nutritional (30 mg/d) levels on Zn, Fe and Cu status and on serum lipid profile in healthy free-living subjects over 55 years old.
The results of the present study show clearly that serum Zn level and Zn urinary excretion responded well to Zn supplementation and thus can be considered as good Zn status biomarkers. The effect of Zn supplementation on Zn status appeared to be dose-dependent. Regarding the effect of Zn supplementation on all subjects (age and sex together), 15 mg Zn/d increased serum Zn level by 8·5 %, whereas 30 mg/d increased serum Zn level by 17·4 %. Urinary Zn excretion also presented a similar pattern (Table 2). The lower limit of fasting plasma Zn level has been set at 10·7 μmol/l (Maret & Sandstead, Reference Maret and Sandstead2006). This is usually considered as the cut-off level below which a Zn-deficient status is possible (Expert Scientific Working Group, Federation of American Societies for Experimental Biology, 1984). Some studies have reported the status of institutionalised (Schmuck et al. Reference Schmuck, Roussel, Arnaud, Ducros, Favier and Franco1996; Artacho et al. Reference Artacho, Ruiz-Lopez, Gamez, Puerta and Lopez1997; Girodon et al. Reference Girodon, Blache, Monget, Lombart, Brunet-Lecompte, Arnaud, Richard and Galan1997) or younger subjects (Coudray et al. Reference Coudray, Richard, Laporte, Faure, Roussel and Favier1992; Rükgauer et al. Reference Rükgauer, Klein and Kruse-Jarres1997) but to our knowledge, plasma reference values of essential trace element status in healthy older subjects have not been yet defined. In the present study, it can be assumed that the observed increase in serum Zn level indicates an improvement in Zn status for this population. This assumption is supported by the statement of reference values considering 15 μmol/l as the mean level of Zn in human plasma as reviewed by Brown (Reference Brown1998) or according to Rükgauer et al. (Reference Rükgauer, Klein and Kruse-Jarres1997) who reported a reference plasma Zn level for a population aged from 22 to 75 years as 16·6 ± 6·2 μmol/l (mean ± 2 sd). Furthermore, Savarino et al. (Reference Savarino, Granchi, Ciapetti, Cenni, Ravaglia, Forti, Maioli and Mattioli2001) hypothesised that a high plasma Zn level in older individuals could contribute to their longevity. The increased plasma Zn level is in agreement with the beneficial effect of Zn supplementation (20 mg/d as combined supplementation) reported in an older institutionalised population presenting a large prevalence of biological Zn deficiency ( < 10·7 μmol/l; Girodon et al. Reference Girodon, Blache, Monget, Lombart, Brunet-Lecompte, Arnaud, Richard and Galan1997). Similarly, a beneficial effect of a higher Zn status (14·7 v. 12 μmol/l) has been reported in an age-related eye disease (Age-Related Eye Disease Research Group, 2002).
The response of serum Zn level and urinary Zn excretion to 30 mg Zn/d supplementation was similar at month 3 and month 6, indicating that Zn supplementation at this dose for 3 months was effective in improving Zn status and decreasing the percentage of subjects with Zn deficiency. In the middle-aged group, all subjects with a serum Zn level < 10·7 μmol/l at baseline (5·2 %) had recovered an adequate serum Zn level >11 μmol/l after 3 months of 30 mg Zn/d supplementation. In the older group, 86 % of individuals had recovered an adequate serum Zn level >11 μmol/l after 3 months' supplementation. Zn supplementation at 15 mg/d was not as effective in increasing serum Zn level in the middle-aged subjects compared with the older group. In agreement with the present results, Bogden et al. (Reference Bogden, Oleske and Lavenhar1988) found no significant change in serum values in response to a 15 mg Zn supplement taken for 3 months. This may be explained by the higher prevalence of a low Zn status in older subjects (5·6 %) than in middle-aged subjects (4·8 %) at baseline (Andriollo-Sanchez et al. Reference Andriollo-Sanchez, Hininger-Favier and Meunier2005). At 6 months, the significant increase in serum Zn level was 16 % for both supplemented groups and reached a similar Zn status observed by Savarino et al. (Reference Savarino, Granchi, Ciapetti, Cenni, Ravaglia, Forti, Maioli and Mattioli2001) in healthy elderly.
Considering the low prevalence (less than 5 %) of Zn intakes below two-thirds European RDA in our studied population at baseline (Andriollo-Sanchez et al. Reference Andriollo-Sanchez, Hininger-Favier and Meunier2005), it was necessary to check if deviations from adequate dietary intakes by supplementation could be detrimental to trace element homeostasis and lipid metabolism. The potential interaction between Fe and Zn has caused concern (Lonnerdal, Reference Lonnerdal2000). The deleterious effect of Fe supplementation on Zn absorption has been well documented, as Fe deficiency is the most common single-nutrient supplementation in the world. Indeed, many findings from metabolic and supplementation studies (Patterson et al. Reference Patterson, Winkelmann and Perry1985; Solomons, Reference Solomons1986) suggest an antagonist relationship between Fe and Zn. As a consequence of chemically similar transport mechanisms, Fe and Zn are thought to compete for absorption (Sandstrom, Reference Sandstrom2001). In the present study, no major and consistent significant negative effects of Zn supplementation on Fe status, assessed by blood Hb, serum Fe, ferritin, and transferrin saturation, were found with Zn at 15 or 30 mg/d during 6 months when the entire cohort was considered as one group (Table 2). These data are in agreement with a recent review article on this topic (Walker et al. Reference Walker, Kordas and Stoltzfus2005). However, differences in the response of Fe parameters to Zn supplementation could be observed if age or sex was considered. Serum ferritin and transferrin saturation were increased in middle-aged but not in older subjects receiving 30 mg Zn/d. A beneficial effect, monitored by a positive correlation, was described between Zn and transferrin saturation, and between Zn and ferritin (Grzegorzewska & Mariak, Reference Grzegorzewska and Mariak2001). Blood Hb decreased only in older subjects receiving 30 mg/d. This observation, that Zn supplementation at 30 mg/d may have more significant effects on Fe status in middle-aged than in older subjects, may be a result of blood Hb level already being low in older subjects and Zn supplementation decreasing it further in this population. In women but not in men, Zn supplementation resulted in a decrease in blood Hb but in an increase in serum Fe, ferritin and transferrin saturation. These apparent contradictory effects may be explained partially by the negative effects of Zn supplementation on serum Cu levels in women that may decrease Hb formation since Cu is well known to participate in Hb synthesis (Hart et al. Reference Hart, Steenbock, Waddell and Elvehjem2002). In turn, this decrease in Hb could spare Fe, which could explain the increase in Fe status in women. To our knowledge, two trials showed an increase in plasma ferritin (Penny et al. Reference Penny, Marin, Duran, Peerson, Lanata, Lonnerdal, Black and Brown2004) and Hb levels (Smith et al. Reference Smith, Makdani, Hegar, Rao and Douglass1999) in Zn-supplemented children.
Zn intake, especially at moderate to high doses, can interfere with Cu utilisation (Sandstead et al. Reference Sandstead, Henriksen, Greger, Prasad and Good1982). It has been previously proposed that Zn could act as a Cu antagonist, inhibiting absorption and mobilisation, which can result in Zn-induced Cu deficiency and consequent anaemia (Sandstrom, Reference Sandstrom2001). However, in the present study, we did not observe any change in serum Cu level when the entire cohort was considered as a single group (Table 2). The absence of an effect of Zn supplementation on Cu status is consistent with the study by Samman & Roberts (Reference Samman and Roberts1987) that tested the effect of 50 mg/d on healthy volunteers over a 6-week period, indicating that increased intakes of Zn do not interfere with plasma Cu status, especially when the population does not exhibit low Cu serum levels. Even if serum Cu is well known as an insensitive marker of Cu status, it is largely used to measure the response of Zn and Cu interaction. Nevertheless, Zn supplementation at 30 mg/d resulted in a decrease in serum Cu level in women, but not in men in the present study. A negative effect of Zn supplementation at 50 mg/d during 2 months in adult females on Fe status and erythrocyte Cu,Zn-SOD activity has been already reported (Yadrick et al. Reference Yadrick, Kenney and Winterfeldt1989). On the contrary, in the present study, erythrocyte SOD activity was increased; the discrepancy between these results could be explained by a lower Zn supplementation in the present study, 30 v. 50 mg/d. This effect on Cu,Zn-SOD activity seems to be age- and sex-dependent. This increase was much more marked in middle-aged than in older subjects and much more in women than in men. The erythrocyte SOD, containing Cu and Zn, is often considered as a biomarker of Cu status, but can be considered as a biomarker of Zn status as well (Coudray et al. Reference Coudray, Richard, Laporte, Faure, Roussel and Favier1992). In support of this is the observed increase in its activity as a response of this enzyme to Zn supplementation in the present study. According to our hypothesis, a positive correlation has been described between Zn and serum SOD activity (Paik et al. Reference Paik, Joung, Lee, Lee, King and Keen1999).
When all subjects were considered, we did not observe major adverse effects of Zn supplementation on serum lipid profile in the present study (Table 2). These data agree with the Age-Related Eye Disease Research Group (2002) study using Zn (80 mg/d) as zinc oxide supplementation in a population aged 55–80 years. The plasma Zn level increased to the same level in the two studies: 14·7 and 14·6 μmol/l in Age-Related Eye Disease Research Group study and the present study (with 30 mg/d), respectively. The higher Zn dose and the larger duration of supplementation could explain these similar results whereas it is well described that zinc oxide has a lower bioavailability (Spiemann et al. Reference Spiemann, Spank, Kluge, Schappach and Kirch2005). It is also possible that at this Zn dose Zn plateaued for this cross-section of age. However, in the present study, lipid parameter responses to Zn supplementation were also age- and sex-dependent. In middle-aged subjects but not in older subjects, Zn supplementation, at the dose of 30 mg/d, resulted in an increase in serum total cholesterol, LDL levels and in the LDL:HDL ratio (Table 3). This may be explained partially by the fact that these parameters were already high in the older subjects and Zn supplementation did not increase them further. In line with this is the observation indicating that the highest quintile of Zn level had been associated with highest levels of total serum cholesterol (Singh et al. Reference Singh, Niaz, Rastogi, Bajaj, Gaoli and Shoumin1998; Hercberg et al. Reference Hercberg, Bertais and Czernichow2005). In women, but not in men, Zn supplementation, at the dose of 30 mg/d, resulted in an increase in serum TAG levels. According to our data, a similar sex-dependent effect of Zn on TAG level was also reported in the SU.VI.MAX study with a multi-nutrient antioxidant supplementation containing 20 mg Zn (Hercberg et al. Reference Hercberg, Bertais and Czernichow2005). Moreover, we did not report a negative effect of Zn supplementation on HDL status, consistent with the results of some (Crouse et al. Reference Crouse, Hooper, Atterbom and Papenfuss1984; Fosmire, Reference Fosmire1990; Hiller et al. Reference Hiller, Seigel and Sperduto1995; Bonham et al. Reference Bonham, O'Connor, McAnena, Walsh, Downes, Hannigan and Strain2003; Hercberg et al. Reference Hercberg, Bertais and Czernichow2005) but not all (Hooper et al. Reference Hooper, Visconti, Garry and Johnson1980; Chandra, Reference Chandra1984; Chevalier et al. Reference Chevalier, Liepa, Murphy, Suneson, Vanbeber, Gorman and Cochran2002) studies. It seems that these results depend on the studied Zn intake, in particular when it is excessive, since in these studies, the adverse effects on HDL were described for pharmacological Zn supplementation at 50 mg/d (Black et al. Reference Black, Medeiros, Brunett and Welke1988; Chevalier et al. Reference Chevalier, Liepa, Murphy, Suneson, Vanbeber, Gorman and Cochran2002) or higher; 75 mg/d (Black et al. Reference Black, Medeiros, Brunett and Welke1988); 300 mg/d (Chandra et al. 1984); 440 mg/d (Hooper et al. Reference Hooper, Visconti, Garry and Johnson1980). Furthermore, men (Crouse et al. Reference Crouse, Hooper, Atterbom and Papenfuss1984; Bonham et al. Reference Bonham, O'Connor, McAnena, Walsh, Downes, Hannigan and Strain2003) seem to be more affected by Zn supplementation on HDL than women (Freeland-Graves et al. Reference Freeland-Graves, Friedman, Han, Shorev and Young1982; Samman & Roberts, Reference Samman and Roberts1988). The mechanism by which Zn interferes with lipid metabolism is not clear but thought to be related to induced Cu deficiency (Scientific Committee of Food, 2003). Regarding the parameters evaluated in the present study, the moderate Zn dose of 15 mg/d could be considered as non-detrimental to health. Considering the risk of adverse effects of Zn supplementation on immunity, reported by Chandra (Reference Chandra1984), the dose was very different, more than ten times higher (300 mg/d) in his study than in ours (15 or 30 mg/d). Indeed, in the present study, we did not observe a toxic effect on immune responses assessed in the Zenith study population (Wallace et al. 2006).
In conclusion, Zn supplementation at 15 or 30 mg/d for 6 months resulted in beneficial effects on serum Zn level and increased Zn urinary excretion. However, these Zn doses did not improve consistently serum alkaline phosphatase activity or erythrocyte Zn level and erythrocyte SOD activity in both sexes and both age groups. The overall effects of Zn supplementation as 15 or 30 mg/d showed no major significant adverse effects on Fe and Cu status, or on lipid metabolism. However, the response of some biochemical parameters to Zn supplementation was age- or sex-dependent. Serum ferritin, percentage transferrin saturation, cholesterol and LDL-cholesterol were increased in middle-aged but not in older subjects receiving 30 mg Zn/d. Moreover, blood Hb decreased in older subjects receiving 30 mg/d. In women, but not in men, Zn supplementation resulted in an increase in serum Fe, ferritin and percentage transferrin saturation as well as in serum TAG and a decrease in blood Hb. These results show clearly that 15 mg Zn/d presented no adverse effect on lipid profile in contrast to 30 mg Zn/d which induced some adverse effects on a subgroup of our population. These observations should be of great use in medical practice and allow the appropriate dose of Zn supplementation for the elderly and highlighting a possible complication attendant to their use. However, bearing in mind that Zn is a constituent of many enzymes and plays a role in many major metabolic pathways, there could be adverse or beneficial effects of oral Zn supplementation that we did not investigate.
Acknowledgements
We thank the subjects for their conscientious compliance with the trial restrictions. The Zenith Study is supported by the European Commission ‘Quality of Life and Management of Living Resources’ Fifth Framework Programme, Contract no: QLK1-CT-2001-00 168. The authors wish to thank Dr E. E. A. Simpson for his help in recruitment at the Coleraine centre.




