A 54-year-old man with decompensated alcoholic cirrhosis was admitted to the hospital with hepatic encephalopathy. Rifaximin, lactulose, albumin infusions, and tube feeds were initiated. Three days after admission, his hemoglobin dropped due to presumed gastrointestinal bleeding, for which he received blood transfusion and bolus normal saline. Electroencephalography 12 days after admission for decreased level of consciousness revealed nonconvulsive status epilepticus, while brain magnetic resonance imaging (MRI) 13 days after admission showed central pontine diffusion restricting signal abnormality resembling a trident (Figure 1A). He was intubated for airway protection and seizure control. Electrographic seizure activity ceased with levetiracetam, clobazam, and propofol. Upon weaning of propofol, seizures did not recur but his level of consciousness was persistently decreased. On examination, his Glasgow Coma Scale was 3T. He was unarousable. Pupils were small and minimally reactive. Corneal reflexes were present. Horizontal eye movements were limited. Gag reflex was not elicitable. His legs were hypertonic and hyperreflexic. There was no withdrawal from painful stimuli. Repeat MRI 19 days after admission showed ventrolateral progression of pontine diffusion restricting signal abnormality with sparing of the corticospinal tracts, resembling a pig’s snout (Figure 1B). Additional signal abnormality of the thalamus, basal ganglia, and frontoparietal cortices was also observed. On chart review, we noted that over the first 6 days of his admission his serum sodium increased from 132 to 161 mmol/L (normal: 135−145 mmol/L), with a maximum 24-h increase of 8 mmol/L. The significant rise in his serum sodium coupled with his radiographic findings was concerning for osmotic demyelination syndrome (ODS). His serum sodium was closely monitored thereafter to avoid further fluctuations. No clinical improvement occurred, and after discussion with his family, comfort care measures were implemented. He passed away 1 month after admission. Autopsy was performed, and Luxol fast blue stain confirmed extensive pontine demyelination that relatively spared the peripheral pons and corticospinal tracts (Figure 1C). Findings compatible with extra-pontine demyelination and acquired hepatocerebral degeneration were also observed.

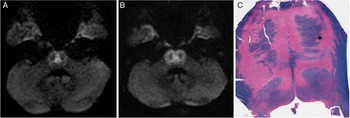
Figure 1: Neuroimaging and pathological depiction of the “pig’s snout” sign in osmotic demyelination syndrome. On serial brain MRI, axial diffusion-weighted imaging (DWI) on day 13 of admission (A) shows central pontine hyperintensity (“trident” sign) that evolved to more extensive pontine hyperintensity (“pig’s snout” sign) on day 19 of admission (B). Corresponding apparent diffusion coefficient map confirmed true diffusion restriction (not shown). On autopsy, Luxol fast blue stain confirmed extensive pontine demyelination that relatively spared the corticospinal tracts (C) as the cause of the pig’s snout appearance.
ODS is typically a complication of treatment of patients with severe hyponatremia. Reference Martin1 However, additional risk factors (e.g., alcoholism, malnutrition, liver disease) may predispose to ODS even with milder degrees of hyponatremia, as in our patient. Reference Martin1 While initially described as a disease of the pons (central pontine myelinolysis), later recognition of lesions outside the pons (extra-pontine myelinolysis) render the broader term ODS more appropriate. Reference Martin1 The precise underlying disease mechanisms are unclear, but demyelination is thought to be due to osmotic stresses causing oligodendrocyte death. Reference Ruzek, Campeau and Miller2 The "trident" sign is a classical neuroimaging finding in ODS that reflects demyelination of crossing pontocerebellar fibers. Reference Ruzek, Campeau and Miller2 In contrast, the “pig’s snout” sign or “piglet” sign has only been rarely reported and refers to larger pontine lesions that extend ventrolaterally while sparing the peripheral pons and corticospinal tracts. Reference Wagner, Mueller-Schunk and Schankin3,Reference Beh4 Progression from the trident sign to the pig’s snout sign in our case supports that they exist on a spectrum of disease severity. Pathological findings in our case confirm that the pig’s snout sign reflects extensive pontine demyelination, further supporting a severe form of ODS. Recognition of the pig’s snout sign can aid in the accurate diagnosis of ODS.
Conflicts of Interest
The authors have no conflicts of interest.
Statement of Authorship
AB: design and conceptualization, data analysis and interpretation, drafting of the manuscript
LCA: data analysis and interpretation, critical revision of the manuscript for intellectual content
DBD: design and conceptualization, data analysis and interpretation, critical revision of the manuscript for intellectual content.