



To the Editor—Clostridioides difficile, formerly known as Clostridium difficile, is a spore-forming anaerobe that is believed to colonize ~5%–10% of healthy adults and is usually asymptomatic.Reference Kato, Kita and Karasawa1 The toxin-producing strains of Clostridioides difficile can cause Clostridioides difficile infection (CDI), which is characterized by frequent diarrhea. CDI is the leading cause of infectious diarrhea in hospitalized patients, and some risk factors of CDI, such as old age, antibiotic use, and proton pump inhibitor (PPI) use have already been reported.Reference Polage, Solnick and Cohen2, Reference Loo, Bourgault and Poirier3 The incidence of CDI is 0.8–4.71 per 10,000 patient days in Japan.Reference Riley and Kimura4 Clostridioides difficile can be widely distributed in the environment as spores, which are extremely resistant to environmental changes including alcohol sterilization; therefore, prompt and appropriate diagnosis of CDI is important for the prevention of nosocomial spread of CDI.
A rapid stool test kit for detecting toxins and glutamate dehydrogenase (GDH) antigen is generally used to diagnose CDI. Although the sensitivity of this kit for the GDH antigen is high (~90%), the sensitivity for the toxins is relatively low; thus, comprehensive assessment is required if toxins are negative. Stool culture is helpful for the diagnosis of CDI in the case of a conflicting result that is positive for the GDH antigen and negative for the toxin test, although it is lengthy and complex to perform. The latest guideline recommended that testing should be performed on patients with the onset of ≥3 instances of diarrhea within 24 hours without any other cause.Reference McDonald, Gerding and Johnson5
Green stool is often considered a clinical indication of suspected CDI. We hypothesized that the color of stool can be a clue used for the diagnosis of CDI; hence, the objective of this pilot study was to assess the relationship between CDI and stool color.
We conducted a prospective observational study at St Luke’s International Hospital, a large academic hospital in Tokyo, Japan, from July 2018 to January 2019. We included all stool samples derived from hospitalized patients who were 18 years old or older and performed a stool test for CDI 72 hours after admission. We excluded those who could not provide written consent prior to entry into this study. All information was extracted from electronic medical records. The St Luke’s International Hospital Ethics Committee institutional review board approved this study (approval no. 18-J005).
We defined CDI according to the following criteria: (1) toxins A and B were positive, or (2) toxins A and B were negative but GDH antigen and stool culture were positive for CDI. Stool samples were divided into 2 groups: patients having CDI (CDI group) and patients without CDI (control group). To detect toxins and GDH antigen, we used C. DIFF QUIK CHEK COMPLETE (Techlab, Blacksburg, VA), an enzyme immunoassay screening kit.
We imaged each stool sample using an EOS Kiss M digital camera (Canon, Tokyo, Japan). The images were color adjusted using Adobe Photoshop CC 2019 (Adobe, San Jose, CA) using CasMatch (Bear Medic, Ibaraki, Japan), a color chart for image correction. Color samples were extracted from 3 points in each color-adjusted image. These color samples were represented in the hue–saturation–value color system. We used the average hue value for statistical assessment of the stool color.
We extracted patient information, including age, gender, vital signs, laboratory data, and use of antibiotics, probiotics, PPI, or tube feeding from medical records. Vital signs on the day the stool sample was collected were investigated to record the maximum axillary temperature, lowest systolic blood pressure, and “shock index” (ie, systolic blood pressure divided by heart rate). Laboratory data collected were white blood cell count (WBC/μL), albumin level, and creatinine level.
We compared the characteristics of the stool samples between the control and the CDI groups. We then compared the stool colors between each group. The Mann-Whitney U test was used for continuous variables, and the Fisher exact test was used for categorical variables. All analyses were performed in January 2019 using R studio version 3.5.0 software (R Foundation for Statistical Computing, Vienna, Austria) and EZR.Reference Kanda6
In total, 84 stool samples were included in this study, and 4 stool samples met the definition of CDI. The median overall age of the case patients was 73 years, and 41 of the positive samples (47.7%) were obtained from women. The proportion of women (p = 0.047) and the patients with ≥15,000 WBC/μL (p < 0.01) in the CDI group were significantly greater than in the control group. The results of univariate analysis of stool color are shown in Figure 1. The median hue value was 30.3° (range, 25.0–49.3) in the CDI group and 41.3° (range, 16.7–88.0) in the control group. A greater tendency to be greenish was observed in the control group rather than the CDI group, although there was no statistically significant difference (p = 0.118).
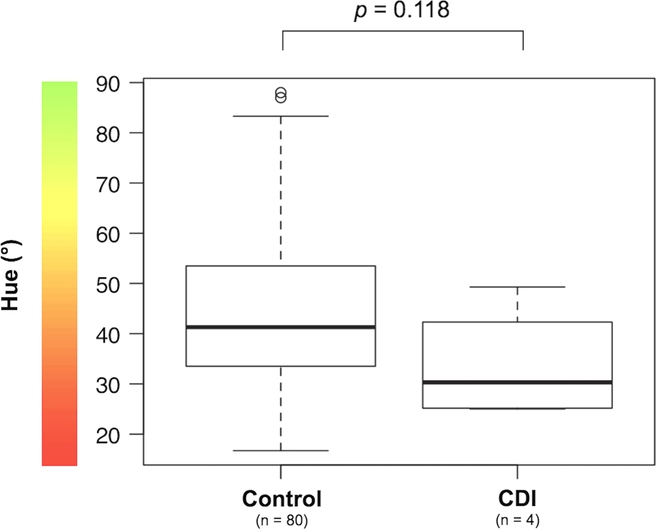
Fig. 1. The results of univariate analysis about stool color. The median hue value was 30.3° (range, 25.0–49.3°) in the Clostridioides difficile infection (CDI) group and 41.3° (range, 16.7–88.0°) in the control group. A greater tendency to be greenish was observed in the control group rather than the CDI group.
In this study, there was no statistically significant difference between stool color and CDI, suggesting that stool color may not contribute to the diagnosis of CDI. On the other hand, whether the patients had ≥15,000 WBC/μL was significantly different in the univariate analysis, and this finding is consistent with previous studies.Reference McDonald, Gerding and Johnson5 This study was a single-center study and the number of stool samples was small. Furthermore, we did not examined other factors that can affect stool color, such as dietary content. Hence, a more detailed investigation with an increased number of stool samples is warranted.
Author ORCIDs
Hiroshi Sugimoto, 0000-0002-2053-8858
Acknowledgments
None.
Financial support
No financial support was provided relevant to this article.
Conflicts of interest
All authors report no conflicts of interest relevant to this article.

