

Introduction
Despite well-documented health disparities among rural residents, they remain underrepresented in clinical research [Reference Ford, Howerton and Lai1]. Although approximately 14% of US residents live in rural areas, only 3% of the National Cancer Institute’s clinical research focused on rural populations between 2011 and 2016 [2,Reference Blake, Moss, Gaysynsky, Srinivasan and Croyle3]. Some factors contributing to this are that rural populations in America face several barriers to healthcare compared to urban and suburban populations, and clinical research studies are often offered as part of medical encounters [Reference Chen, Orom and Hay4]. Barriers to accessing healthcare in rural communities include geographical distances to medical facilities requiring extensive travel and lodging costs, lack of public transportation, stigma, and distrust of the healthcare system [Reference Golembiewski, Gravholt and Torres Roldan5,Reference Davis, Arnold, Mills and Miele6]. Representation of rural populations in clinical research is necessary to understand and deploy effective health care strategies that can benefit all rural individuals, increasing the generalizability and equity of research findings.
Recently, developing infrastructure and capabilities for clinical research to address health disparities among rural populations has been viewed as a national priority [Reference Temple7,8]. In response, collaborative efforts involving community-academic partnerships on community engagement, late-stage translation, and digital infrastructure have begun to address the inadequate digital infrastructure and barriers to health care access among rural communities [Reference Leppin, Mahoney and Stevens9,10]. A body of evidence showed that recruitment and participation of rural populations can be facilitated through community engagement in research [Reference Julian McFarlane, Occa, Peng, Awonuga and Morgan11,Reference Baquet, Bromwell, Hall and Frego12]. Collaboration with community members has numerous merits including addressing prevalent health issues, strengthening researchers’ understanding of community priorities, and supporting culturally appropriate communication [Reference Wieland, Njeru, Alahdab, Doubeni and Sia13]. However, evidence for a comprehensive understanding of specific strategies for promoting participation in clinical research among residents of rural communities is unclear.
The goal of this narrative review is to evaluate the extant literature about the use of community engagement strategies to promote recruitment, enrollment, and participation in clinical research with rural communities. This review will highlight effective strategies in promoting participation and identify ineffective ones. This knowledge will progress the current understanding of the issue and outline specific strategies that can be applied in clinical research based in rural settings.
Methods
To achieve the proposed objective, a narrative review was used to address the knowledge gap on ways to engage and promote clinical research in rural communities. This narrative review followed the PRISMA-ScR guidelines to plan, conduct, and report the results [Reference Tricco, Lillie and Zarin14].
Data Sources and Search Strategies
Online searches were conducted using a variety of different strategies with assistance from an experienced medical librarian. We searched PubMed, Embase, CINAHL, Scopus, Web of Science, and Cochrane Database of Systematic Reviews to identify English-language manuscripts about clinical research among rural communities. Searches of ClinicalTrials.gov were conducted to capture unpublished or ongoing research. A variety of keywords, some truncated, and subject headings were combined using Boolean operators to retrieve results in the databases. The searches included terms such as “community engaged research,” “CEnR,” “rural populations,” “recruitment,” “intervention,” “research subjects,” and “patient selection.” Results were restricted to human subjects and clinical research publication type.
Study Eligibility and Outcome Measures
In this review, studies were eligible for inclusion if they included community engagement approaches, recruitment, and enrollment of rural participants to clinical research in the United States. Clinical research was defined as “A component of medical and health research intended to produce knowledge valuable for understanding human disease, preventing and treating illness, and promoting health” [15]. Key components included a sponsor, study question, study population, inclusion/exclusion criteria, observation and/or intervention, and outcomes. Types of research studies included were bi-directional integrative (translational) research, community-based clinical research, therapeutic interventions, prevention and health promotion, behavioral research, and health services research. Exclusion criteria were non-English articles, studies conducted outside the United States, systematic reviews, non-original research, and did not include rural populations. In some strategies, the text words and publication types “systematic reviews” and “meta-analyses” were also excluded. No publication period restrictions were applied to the database searches (Table 1).
Table 1. Summary of inclusion and exclusion criteria for the narrative review

Screening and Data Extraction
All records were screened among two-three reviewers by title and abstract, full text, and data extraction. Covidence was used for all study screening and data extraction activities. For data extraction and synthesis, three reviewers were assigned to each article, with decisions based on agreement among two-three of the reviewers. The following items were extracted from these studies: study design, study focus (recruitment, retention, or both), study population(s), study setting(s), number of rural research participants recruited, study description/aim, community engagement intervention for rural recruitment, level of community engagement, and major findings from the study.
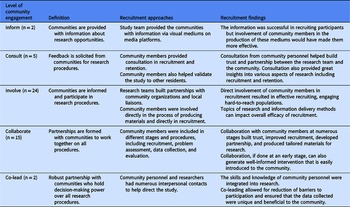
The International Association for Public Participation’s Spectrum of Public Participation [16] broadly categorizes community engagement; thus, the levels of community engagement were adapted and defined as follows: (1) inform – communities are provided with information about research opportunities, (2) consult – feedback is solicited from communities for research procedures, (3) involve – communities informed and participate in research procedures, (4) collaborate – partnerships are formed with communities to work together on all procedures, and (5) co-lead – robust partnership with communities who hold decision-making power over all research procedures. If applicable, the number of urban participants was also extracted from the study. All data extraction, synthesis, and consensus were captured in Covidence for summarizing and comparisons.
Synthesis of Results
Following the data extraction process, the information gathered was coded for the following: strategies that worked to recruit participants, strategies that did not work to recruit participants, and recruitment findings/outcomes. Three reviewers were involved in this process, and the data were then combined for one final consensus.
Results
Search Results
Database searches retrieved a total of 3382 papers, which yielded 2473 unique papers after de-duplication. In screening the titles and abstract, 2068 articles were excluded because of irrelevant populations, study type, setting, or missing abstract. After further screening, investigators then reviewed 405 papers of which forty-eight articles were identified to have fulfilled the inclusion criteria (see Fig. 1).

Fig. 1. PRISMA flow diagram.
Characteristics of Included Studies
The included studies were published between 1990 and 2021. Of the forty-eight articles, almost half (41.7%) were randomized controlled trials, and a third were quasi-experimental studies (27.1%). The remaining articles included mixed methods (8.3%), cohort designs (8.3%), cross-sectionals (8.3%), non-randomized clinical research (2.1%), case studies (2.1%), and stratified random sample studies (2.1%). The majority (91.7%) focused on rural communities, and the remaining (8.3%) included both rural and urban communities. The bulk of the included articles (70.8%) either focused on or included underrepresented groups including African American, Hispanic, American Indian or Alaska Native (AIAN) or Asian people, or the transgender community. The health-related themes of forty-eight articles were diverse; however, these were clustered into five categories: nutrient-related and nutrient processing problems (39.6%), cancer (29.2%), behavioral and physical health (27.1%), cardiovascular issues (16.7%), patient engagement (6.3%), and mental health (2.1%). Although there are some articles that only emphasized one health disparity, some had multiple. Over two-thirds (68.8%) were conducted in community settings, while 18.8% were in clinical settings and 18.8% at home or by phone. Two studies were conducted in multiple settings (Table 2).
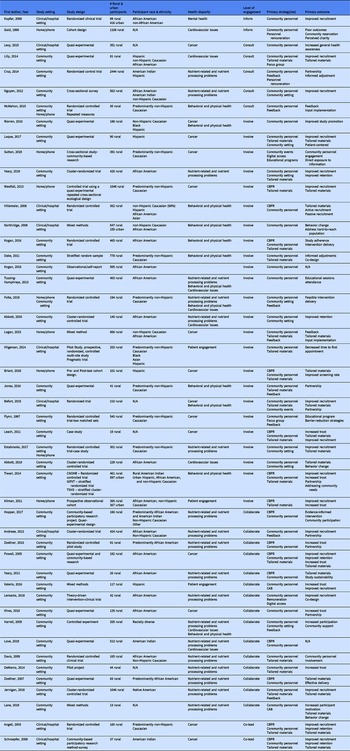
Table 2. Characteristics of selected articles

Recruitment Strategies
All the studies were examined in four categories: recruitment strategies, recruitment strengths, recruitment limitations, and findings (Table 3). Of the forty-eight articles included, thirty-one had a study focus on recruitment. Most of these relied on community engagement for successful recruitment of research participants. Involvement of community personnel (n = 46) [Reference Warren, Maley, Sugarwala, Wells and Devine17–Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62], feedback (n = 22) [Reference Hopper, Blackman and Page18,Reference Andreae, Halanych, Cherrington and Safford20,Reference Zoellner, Hill and Grier23,Reference Angell, Kreshka and McCoy25,Reference Westfall, Zittleman and Sutter26,Reference KH-cK, Cornell and Moore31,Reference Dake, Price, McKinney and Ward32,Reference Lilly, Bryant and Vu34,Reference Folta, Paul and Nelson38,Reference Cruz, Davis, FitzGerald, Canaca and Keane42–Reference Logan, Guo and Emanuel45,Reference Davis, Hitch, Nichols, Rizvi, Salaam and Mayer-Davis49,Reference Zoellner, Connell and Santell51–Reference McMahon, Wyman, Belyea, Shearer, Hekler and Fleury53,Reference Jones, Starcher, Eicher and Wilcox55–Reference Flynn, Gavin, Worden, Ashikaga, Gautam and Carpenter57,Reference Tiwari61,Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62], and customization of recruitment materials and processes in accordance with the characteristics of the community (n = 17) [Reference Luque, Tarasenko and Reyes-Garcia19,Reference Yeary, Moore and Gauss22,Reference Angell, Kreshka and McCoy25–Reference Powell, Carter and Bonsi27,Reference Dake, Price, McKinney and Ward32,Reference Lilly, Bryant and Vu34,Reference Logan, Guo and Emanuel45,Reference Hilgeman, Mahaney-Price and Stanton47–Reference De Marco, Kearney, Smith, Jones, Kearney-Powell and Ammerman50,Reference Jernigan, Williams and Wetherill52,Reference Befort, Bennett, Christafano, Klemp and Krebill56,Reference Leach, Schoenberg and Hatcher58,Reference Tiwari61,Reference Allman, Sawyer, Crowther, Strothers, Turner and Fouad63] were mentioned most frequently. Some other recruitment strategies included providing remuneration (either for participants or for community personnel) (n = 14) [Reference Luque, Tarasenko and Reyes-Garcia19,Reference Zoellner, Hill and Grier23,Reference KH-cK, Cornell and Moore31,Reference Kogan, Cho and Oshri33,Reference Valerio, Rodriguez and Winkler35,Reference Lemacks, James and Abbott37,Reference Cruz, Davis, FitzGerald, Canaca and Keane42,Reference Love, Taniguchi and Williams44,Reference Briant, Sanchez and Ibarra48,Reference Davis, Hitch, Nichols, Rizvi, Salaam and Mayer-Davis49,Reference Zoellner, Connell and Santell51,Reference Gold and Franks54,Reference Leach, Schoenberg and Hatcher58,Reference Tiwari61] and utilizing local spaces and events (n = 15) [Reference Luque, Tarasenko and Reyes-Garcia19,Reference Sutton, Preston and Thomson21,Reference Yeary, Moore and Gauss22,Reference Hillemeier, Downs and Feinberg28–Reference Kogan, Lei, Brody, Futris, Sperr and Anderson30,Reference Folta, Paul and Nelson38,Reference Abbott, Slate and Graven39,Reference Cruz, Davis, FitzGerald, Canaca and Keane42,Reference Nguyen, Arcury and Grzywacz46,Reference Befort, Bennett, Christafano, Klemp and Krebill56,Reference Leach, Schoenberg and Hatcher58–Reference Abbott, Williams, Slate and Gropper60,Reference Allman, Sawyer, Crowther, Strothers, Turner and Fouad63]. Although the majority of articles did not discuss limitations of the recruitment strategies, a few mentioned some challenges, including issues regarding community personnel recruitment [Reference Jones, Starcher, Eicher and Wilcox55,Reference Tiwari61], community personnel turnover [Reference Andreae, Halanych, Cherrington and Safford20,Reference Tiwari61], study interval [Reference Gold and Franks54], absence of educational programs [Reference Gold and Franks54], and ineffective recruitment via faith-based organizations [Reference Jones, Starcher, Eicher and Wilcox55]. Numerous outcomes of the recruitment strategies were discussed, most of which were positive. Among all the findings, production of tailored materials and procedures (n = 17) [Reference Luque, Tarasenko and Reyes-Garcia19,Reference Angell, Kreshka and McCoy25–Reference Hillemeier, Downs and Feinberg28,Reference KH-cK, Cornell and Moore31,Reference Lilly, Bryant and Vu34,Reference Logan, Guo and Emanuel45,Reference Briant, Sanchez and Ibarra48,Reference Zoellner, Connell and Santell51,Reference Jernigan, Williams and Wetherill52,Reference Befort, Bennett, Christafano, Klemp and Krebill56,Reference Leach, Schoenberg and Hatcher58–Reference Abbott, Williams, Slate and Gropper60,Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62,Reference Lane, Porter, Hecht, Harris and Zoellner64], improved participant recruitment (n = 19) [Reference Luque, Tarasenko and Reyes-Garcia19,Reference Andreae, Halanych, Cherrington and Safford20,Reference Yeary, Moore and Gauss22,Reference Angell, Kreshka and McCoy25–Reference Powell, Carter and Bonsi27,Reference Lilly, Bryant and Vu34,Reference Valerio, Rodriguez and Winkler35,Reference Lemacks, James and Abbott37,Reference Kupfer, Axelson and Birmaher41,Reference Harrell, Davy, Stewart and King43,Reference Nguyen, Arcury and Grzywacz46,Reference Jernigan, Williams and Wetherill52,Reference Befort, Bennett, Christafano, Klemp and Krebill56,Reference Leach, Schoenberg and Hatcher58,Reference Estabrooks, You, Hedrick, Reinholt, Dohm and Zoellner59,Reference Tiwari61–Reference Allman, Sawyer, Crowther, Strothers, Turner and Fouad63], building partnership (n = 9) [Reference Andreae, Halanych, Cherrington and Safford20,Reference Zoellner, Hill and Grier23,Reference Powell, Carter and Bonsi27,Reference Vines, Hunter, White and Richmond40,Reference Cruz, Davis, FitzGerald, Canaca and Keane42,Reference Davis, Hitch, Nichols, Rizvi, Salaam and Mayer-Davis49,Reference Jones, Starcher, Eicher and Wilcox55,Reference Befort, Bennett, Christafano, Klemp and Krebill56,Reference Tiwari61], and increased trust (n = 8) [Reference Zoellner, Hill and Grier23,Reference Powell, Carter and Bonsi27,Reference Valerio, Rodriguez and Winkler35,Reference Vines, Hunter, White and Richmond40,Reference De Marco, Kearney, Smith, Jones, Kearney-Powell and Ammerman50,Reference Leach, Schoenberg and Hatcher58,Reference Tiwari61,Reference Allman, Sawyer, Crowther, Strothers, Turner and Fouad63] were the most commonly observed outcomes. Additionally, there were other noteworthy outcomes: seven studies discussed improved participant retention [Reference Yeary, Moore and Gauss22,Reference Angell, Kreshka and McCoy25,Reference Powell, Carter and Bonsi27,Reference Abbott, Slate and Graven39,Reference Leach, Schoenberg and Hatcher58,Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62,Reference Allman, Sawyer, Crowther, Strothers, Turner and Fouad63], five studies successfully addressed community needs [Reference Jernigan, Williams and Wetherill52,Reference Flynn, Gavin, Worden, Ashikaga, Gautam and Carpenter57,Reference Tiwari61,Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62,Reference Lane, Porter, Hecht, Harris and Zoellner64], and five studies effectively encompassed hard-to-reach populations [Reference Hillemeier, Downs and Feinberg28,Reference Northridge, Vallone and Xiao29,Reference Kupfer, Axelson and Birmaher41,Reference Befort, Bennett, Christafano, Klemp and Krebill56,Reference Leach, Schoenberg and Hatcher58].
Table 3. Levels of community engagement for recruitment

Levels of Rural Community Engagement
Inform
Among the 48 articles, only 2 involved the community at the “inform” level [Reference Kupfer, Axelson and Birmaher41,Reference Gold and Franks54]. Both studies utilized visual mediums as methods of recruitment, specifically TV ads in Kupfer’s article and community presentations in Gold’s article. Although Kupfer’s study was successful in engaging African American population [Reference Kupfer, Axelson and Birmaher41], Gold identified three shortcomings in that study including initial failure to involve community members to produce tailored educational materials, an absence of ongoing educational programs, and the short interval of the study [Reference Kupfer, Axelson and Birmaher41].
Consult
There were five studies identified as engaging the community at the “consult” level [Reference Lilly, Bryant and Vu34,Reference Cruz, Davis, FitzGerald, Canaca and Keane42,Reference Nguyen, Arcury and Grzywacz46,Reference McMahon, Wyman, Belyea, Shearer, Hekler and Fleury53,Reference Levy, Cohen-Louck and Bonny-Noach65]. The community members provided different types of support to the research teams. Although in one study, the recruited community leaders helped validate the legitimacy of the research to elder participants of the community, another demonstrated the effectiveness of a focus group which helped inform the various aspects of the intervention including acceptability, marketing, content, and environment [Reference Lilly, Bryant and Vu34,Reference Nguyen, Arcury and Grzywacz46]. The articles reported some major advantages of engaging the community members in consultation. Cruz maintained that involvement of community members who advocated for the project served to build a foundation of trust and to ensure equity in the partnership, while McMahon noted that the community partners provided advice of great value regarding maximizing participant recruitment and retention [Reference Cruz, Davis, FitzGerald, Canaca and Keane42,Reference McMahon, Wyman, Belyea, Shearer, Hekler and Fleury53].
Involve
Involvement was identified as the level of engagement in half of the studies (n = 24) [Reference Warren, Maley, Sugarwala, Wells and Devine17,Reference Luque, Tarasenko and Reyes-Garcia19,Reference Sutton, Preston and Thomson21,Reference Yeary, Moore and Gauss22,Reference Westfall, Zittleman and Sutter26,Reference Hillemeier, Downs and Feinberg28–Reference Kogan, Lei, Brody, Futris, Sperr and Anderson30,Reference Dake, Price, McKinney and Ward32,Reference Kogan, Cho and Oshri33,Reference Tussing-Humphreys, Thomson, Mayo and Edmond36,Reference Folta, Paul and Nelson38,Reference Abbott, Slate and Graven39,Reference Logan, Guo and Emanuel45,Reference Hilgeman, Mahaney-Price and Stanton47,Reference Briant, Sanchez and Ibarra48,Reference Jones, Starcher, Eicher and Wilcox55–Reference Tiwari61,Reference Allman, Sawyer, Crowther, Strothers, Turner and Fouad63]. In most of these studies, the research teams developed partnerships with local organizations or recruited community personnel and liaisons. These community partners provided insights into the study processes and materials, as well as managing and executing the recruitment process. By employing local members as study staff in the recruitment, populations that would be otherwise unable to reach were engaged in the study due to the increased trust among community members, as observed in Leach’s success in involving rural Appalachian women [Reference Leach, Schoenberg and Hatcher58]. Furthermore, the community partners also helped in tailoring materials and processes to address the communities’ specific needs and characteristics, further improving the effectiveness of recruitment. However, it must be noted that there are some limitations to involving communities to participate in the research procedures. Leach outlined that the effectiveness of community partners recruiting participants was greatly reduced due to the topic of cancer, which was too frightening, especially for those who had experienced loss of loved ones due to cancer. Moreover, some recruitment mediums in the community including emails, paid newspaper advertisements, community flyers, and postcards have also been illustrated to lack efficacy in recruiting participants [Reference Estabrooks, You, Hedrick, Reinholt, Dohm and Zoellner59].
Collaborate
Collaboration was the level of community engagement in fifteen articles [Reference Hopper, Blackman and Page18,Reference Andreae, Halanych, Cherrington and Safford20,Reference Zoellner, Hill and Grier23,Reference Powell, Carter and Bonsi27,Reference KH-cK, Cornell and Moore31,Reference Valerio, Rodriguez and Winkler35,Reference Lemacks, James and Abbott37,Reference Vines, Hunter, White and Richmond40,Reference Harrell, Davy, Stewart and King43,Reference Love, Taniguchi and Williams44,Reference Davis, Hitch, Nichols, Rizvi, Salaam and Mayer-Davis49–Reference Jernigan, Williams and Wetherill52,Reference Lane, Porter, Hecht, Harris and Zoellner64]. In these studies, community members were involved in numerous phases of the research, including problem assessment, recruitment, data collection, and evaluation. The results of collaboration with community members were quite positive. Some of the benefits of collaboration with community personnel include increased trust, improved participant recruitment, partnership between the research group and the locals, production of specialized materials and processes, and addressing the needs of the community. Furthermore, Hopper and colleagues [Reference Hopper, Blackman and Page18] showed that early dedication of time and resources to engage community participation generated well-informed intervention and procedures, both of which were more easily accepted and effectively disseminated within the community.
Co-lead
Co-leading is the driving principle regarding community personnel in only two studies [Reference Angell, Kreshka and McCoy25,Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62]. In Angell’s study, the skills and knowledge of community personnel were integrated into the model which produced numerous interpersonal contacts between recruiters and potential participants and received great advocacy from the community [Reference Angell, Kreshka and McCoy25]. In Schroepfer’s research, the community leaders who had expressed interest in the study met with university partners to assess the study’s accuracy, cultural appropriateness, and other related areas including questions involving insurance [Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62]. The findings from these two articles maintained that the presence of community members in every step greatly reduced barriers to participation and ensured that the data collected was distinct and bore benefits to the community, adhering to the standards of equitable and ethical research.
Discussion
This review unveiled a body of literature regarding the use of community engagement strategies in research conducted in rural populations. The engagement of community members in research was shown to be of great benefit to study recruitment, participant participation, building partnership and trust with the community, and creation of materials and processes tailored to the community’s specific characteristics. Furthermore, engagement of community personnel in the research team ensured that the research was relevant to the community, addressed its specific needs, and benefited the community with its results. This idea of involving community members in the research team has recently been highlighted by existing health programs. A survey conducted in 2011 of the Clinical and Translation Science Awards programs demonstrated that 89% of the projects engaged Community Advisory Boards [Reference Wilkins, Spofford and Williams66]. Thus, it can be maintained that the role of community engagement in research is crucial and is becoming increasingly better acknowledged within the scientific community.
The majority of studies utilized community partners to inform the research regarding recruitment, study materials, and dissemination of the intervention. Different levels of engagement imply different impacts by the community members on the research. Involvement of community personnel is most effective in the recruitment stage in which either the members provide advice on appropriate strategies, directly recruit participants, or serve as a connection between research members and residents of the community [Reference Logan, Guo and Emanuel45,Reference Hilgeman, Mahaney-Price and Stanton47]. The presence of community members in this stage has been shown to greatly increase participant recruitment, as well as retention in some studies [Reference Allman, Sawyer, Crowther, Strothers, Turner and Fouad63]. Moreover, involvement of community members in the research team can also foster increased trust between the researchers and the community participants [Reference Leach, Schoenberg and Hatcher58], which is critical to facilitating effective intervention and access to hard-to-reach populations [Reference Emmel, Hughes, Greenhalgh and Sales67].
Although it was not included in the original inclusion criteria, partnership with local organizations, which is essential in establishing relationships in rural communities, was mentioned in 29 studies [Reference Warren, Maley, Sugarwala, Wells and Devine17,Reference Hopper, Blackman and Page18,Reference Yeary, Moore and Gauss22,Reference Levy, Wolff, Niles, Morehead, Xu and Daly24,Reference Westfall, Zittleman and Sutter26–Reference Northridge, Vallone and Xiao29,Reference Dake, Price, McKinney and Ward32,Reference Valerio, Rodriguez and Winkler35–Reference Harrell, Davy, Stewart and King43,Reference Hilgeman, Mahaney-Price and Stanton47,Reference Briant, Sanchez and Ibarra48,Reference De Marco, Kearney, Smith, Jones, Kearney-Powell and Ammerman50–Reference Jernigan, Williams and Wetherill52,Reference Jones, Starcher, Eicher and Wilcox55,Reference Befort, Bennett, Christafano, Klemp and Krebill56,Reference Estabrooks, You, Hedrick, Reinholt, Dohm and Zoellner59–Reference Tiwari61,Reference Lane, Porter, Hecht, Harris and Zoellner64]. The majority of partnerships were formed with faith-based organizations (70%) and/or local health-related facilities (55%). Additionally, some other organizations involved as partners in the research were local businesses, schools or educational institutions, and general local community organizations. The importance of engaging with rural community-based organizations as a method of promoting research participation has been noted in various literature [Reference Alvarez, Vasquez, Mayorga, Feaster and Mitrani68–Reference Clauser, Johnson, OʼBrien, Beveridge, Fennell and Kaluzny70], as well as the CDC’s Principles of Community Engagement [71]. Culturally appropriate designs and trust in the research are important factors in engaging with the community [Reference Spears, Nolan, O’Neill, Arcury, Grzywacz and Feldman72], which can be facilitated through partnering with community-based organizations and receiving feedback from them. Through building solid relationships with existing local organizations, researchers can familiarize the research to a body of residents and help spread information about the project within the community. Because the majority of the selected papers did not explore the theme of participation engagement exclusively, more research exploring the effects of partnership with community-based organizations is warranted.
Successful recruitment observed in numerous studies was mostly attributed to the engagement of community members who advocated for the study. Most of the studies employed involvement and collaboration as the strategies to engage the community. Compared to information and consultation, collaboration, and involvement transfer some of the decision-making ability to the community members, as they can directly make decisions that impact the studies, evoking a sense of ownership and responsibility toward the research. In a corporate setting, involving employees in the decision-making process can induce a sense of ownership, produce an alignment of interest, and improve overall productivity and quality [Reference Javed and Idris73]. In the setting of clinical research, this can translate into improvement of the quality and effectiveness as observed in the selected articles. Additionally, with more power, community members can positively influence the procedures, strategies, and materials to ensure they best address and benefit the members of the community.
Of the forty-eight studies, only two employed co-leadership as the method of community engagement; however, the findings were very promising. In Angell’s article, efforts made by the community and their input were depicted as indispensable components to the research’s success. Moreover, Schroepfer’s study demonstrated that co-leadership empowered the community, enhanced the capacity of conducting research, and allowed for interpretation of data within the framework of local knowledge, available resources, specific values and beliefs [Reference Angell, Kreshka and McCoy25,Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62]. These positive results certainly highlight the need for future research employing co-leadership as the engagement principle. Notably, both community personnel recruitment and turnover were mentioned as some of the potential challenges of this approach to consider in future research.
Only seven of the studies focused on implementing community engagement strategies among American Indian and Alaska Natives (AIAN) persons [Reference Hopper, Blackman and Page18,Reference Cruz, Davis, FitzGerald, Canaca and Keane42,Reference Love, Taniguchi and Williams44,Reference Nguyen, Arcury and Grzywacz46,Reference Jernigan, Williams and Wetherill52,Reference Tiwari61,Reference Schroepfer, Matloub, Creswell, Strickland and Anderson62]. This is important to consider as AIAN communities remain disproportionately rural compared to other groups, with 29% identified as living in rural areas in 2010 compared to 15% of the total US population [74]. Comprising a large part of rural communities, AIAN people must be included in clinical research in order to learn effective community engagement strategies within this population. Moreover, community engagement techniques may be particularly beneficial when working with AIAN people due to research historically often not addressing community priorities and with little regard for cultural practices [Reference Saunkeah, Beans, Peercy, Hiratsuka and Spicer75]. Furthermore, research has often been done without seeking consent from Indigenous communities or not communicating clearly when obtaining consent [Reference Fitzpatrick, Martiniuk, D’Antoine, Oscar, Carter and Elliott76]. Recent initiatives have called for the need for more culturally sensitive and collaborative approaches in research with indigenous populations [Reference Datta77,Reference Walters and Simoni78]. Community engagement strategies could provide a necessary framework for such efforts; however, more research is needed to better understand best practices within this population.
There are several limitations to the present review. While each level of engagement demonstrated unique benefits to the research, none of the included studies directly compared the different levels of engagement. In future research, it will be beneficial to understand the context in which each level would yield the highest contribution to the successes of the study. Furthermore, knowledge of different engagement principles will also determine balancing community involvement in decision-making and maintaining scientific vigor. Our narrative review is limited to research conducted in the United States and studies published in the English language, limiting generalizability to other countries and languages. Future narrative reviews that include international studies are needed to learn from the work of our neighbors and international partners such as Australia and Canada, who are working on similar issues. Moreover, this review highlights that compared to the whole, CEnR with rural populations occupy only a small portion of the existing body of research. Hence, more CEnR is needed in rural settings that are often underrepresented in the scientific world [Reference Chen, Orom and Hay4]. Additionally, specific definitions and characteristics of rurality were not captured in the present review (e.g., town size). Rurality is a multidimensional concept, and there is great variation across rural communities that need to be considered when implementing community engagement strategies.
Conclusion
This review highlighted the sizeable contributions community members and community leaders can have to the success of research. Most of the studies used collaboration and involvement as the principle driving community engagement. It can be easily observed that including community members on the research staff can enhance the quality of the research, appropriateness of the materials, and effectiveness of intervention delivery. Although it contains many benefits, community engagement is not the omnipotent answer to tackle every barrier, such as transportation, geological isolation, or insufficient services and infrastructure, all of which contribute to the exclusion of rural populations in clinical research. However, it is a necessary component to include in any solution to resolve these issues. Community engagement strategies produce more equity in clinical research, as the participants are part of the team and can ensure that the research is appropriate and beneficial to community. Additional research on community-engaged strategies to enhance clinical research participation among rural populations is warranted [Reference Chen, Orom and Hay4].
Acknowledgements
This publication was supported by Grant Number UL1 TR002377 from the National Center for Advancing Translational Sciences (NCATS). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Disclosures
The authors have no conflict of interest to disclose.



 Open access
Open access