


Online learning is a tool for teaching and assessing students but to date it has been under-utilised in psychiatry. This article outlines the evidence base for such approaches and gives an illustrative account of developing modules for medical undergraduates on the topic of alcohol use and misuse. This may act as a guideline for the development of other psychiatric teaching modules.
Computer-assisted learning
Current medical students have grown up with computers and expect learning materials to be available electronically. The use of computers in medical education is a rapidly expanding field, with systems evolving from simple computer storage of lecture notes to sophisticated web-based multimedia interactive computer-assisted learning modules. An emerging approach is the case-based model, where specific clinical problems are presented using audio and video materials, including laboratory, pathology and radiology findings, with animations, games, quizzes and immediate feedback on performance to sustain interest.
Sporadic developments in computer-assisted learning have been made possible by improvements in information technology and the input of enthusiasts encouraged by positive responses from students (Reference Reid, Harvey and LuqmaniReid et al, 2000). Reviewing the literature, Greenhalgh (Reference Greenhalgh2001) found that prospective randomised controlled trials in this field were too few and too varied in methodology to permit meta-analysis. Nevertheless, such learning packages were at least as effective as conventional teaching formats, and in some cases achieved similar results at less cost of student time. However, not all students are confident or interested in working with computers; moreover the evidence base for cost-effectiveness is sparse. Psychiatrists have not been prominent in this field (Reference LetterieLetterie, 2003) and may thereby miss a valuable teaching opportunity, particularly for integrating areas of psychiatry into other fields of medicine. With increasing student numbers and decreasing numbers of in-patients, there are few patients for student teaching, and developing banks of virtual cases can help to address this need.
Planning
The development of high quality computer-assisted learning modules requires a team that includes educators to help plan learning outcomes and methods of assessment, clinicians to select and provide content, and creative technicians to optimise visual impact and transform content into a variety of interactive elements. The team has to meet regularly, to share ideas, check on progress and maintain the momentum (Reference HuangHuang, 2005). Potential authors will find that looking at the work of others is a guide to what is possible with today's technology. For contributors, the matter of intellectual property must be clear from the outset and in universities the usual practice is for authors to receive acknowledgement but not rights to royalties from the use of materials produced though multimedia departments. Commitment of time is required, although National Health Service (NHS) employers may well be unlikely to give consultants extra sessions to do this work. The university may be persuaded to finance the project, in particular the technician's time. Given the already crowded undergraduate curriculum, it is necessary to consult with those charged with overseeing existing courses so that proposed online learning modules can be integrated into the curriculum.
Educational principles
Educational principles must be given priority and include:
-
• relevance, reliability and validity of content
-
• clarity of delivery
-
• effective use of time
-
• appropriate assessment.
Medical students are strategic learners who will prioritise content that will feature in their examinations (Reference Reid, Duvall and EvansReid et al, 2005). Each module should address four to six main learning outcomes which are selected to concentrate on key clinical topics, particularly where technology can assist students in addressing difficult concepts. Students should be directed to complete the modules at the relevant point in the curriculum, and periods should be timetabled when computers with internet access are available. Students may work individually, although many prefer to work in pairs or threes, which they find enriches the learning experience.
For each module, as with any educational activity, the rule of thumb is to repeat information three times then check for understanding. Students, like patients, can be switched off both by being told at length what they already know or by being overwhelmed by too much information. So, having stated the learning objectives, the minimum requirements should be to establish what the student already knows, deliver the content and offer at least a final test. A reference list and printable summary, including the student's own assessment of what they learned, may also add value (Cranfield Knowledge Garden; http://ollkg.rmcs.cranfield.ac.uk).
Content
Case histories
The use of case histories is a well established approach, with the patient presenting with problems that are investigated: highlighting aspects of basic science before proceeding to management. Some computer-assisted learning modules have used the images and stories of real patients with their consent (Reference D'Alessandro, Lewis and D'AlessandroD’Alessandro et al, 2004). Clinicians may consider creating their own library, using a digital camera and keeping a supply of consent forms available. However, there is no absolute guarantee of online privacy, so to attempt to preserve anonymity, tools such as Adobe Photoshop can be used to remove identifying features of patients such as tattoos. Edinburgh University uses volunteer simulated patients and the modules are held in a secure internet site which overcomes many of the issues relating to confidentiality.
Technical considerations
As with Microsoft PowerPoint presentations, the content on each screen page should be pared down; reading large blocks of text is difficult and it is best to avoid users having to scroll down. Currently, NHS computers block the ‘ streaming’ of video material so it may be preferable to use only still photographs and brief ‘sound bites’ to allow students to run the modules when on placement.
Interactive elements
To sustain attention and interest, it is preferable to interpolate every couple of pages of plain text with quizzes, tables, flow charts and animated diagrams. Students value variety, for example matching names with processes/diagnoses, using short questions with model answers and answering multiple-choice questions. It is most useful to give brief explanations of answers, not simple statements of true or false. The mind is most willing to take on new material at the point it has discovered it did not know. To encourage the curious student, relevant internet links can be included, but these have to be checked regularly to ensure they remain ‘live’. For the purposes of refining modules during production, it is important to ask colleagues and students to give feedback.
Our project–alcohol use and misuse
Alcohol is still the nation's favourite drug and an increasing source of morbidity and mortality among the general population as well as doctors and students (Royal College of Psychiatrists, 1987; Reference PlantPlant, 2004). Alcohol use can lead to or complicate presentations in any speciality and so must be addressed at many points in the medical course. Since the General Medical Council's 1993 report, Tomorrow's Doctors, medical schools have sought to further integrate clinical and non-clinical teaching, and interactive computer-based learning has assisted this process.
E.H.H. became involved in the development of computer-assisted learning modules after attending a course in medical education at the regional postgraduate centre, and subsequently identified another interested specialist registrar (C.E.M.). An analysis of the problems and issues arising from alcohol misuse suggested that at least a dozen modules were required to cover the whole range of alcohol-related morbidities in the short and long term. Moreover, to dispel the stigmatising stereotype that patients with substance misuse are impervious to medical intervention patients with good outcomes would be included. We therefore mapped out a virtual soap opera: a series of case studies based on a group of people who met at a wedding, covering:
-
• social costs
-
• alcohol metabolism
-
• recommended limits and dependence syndrome
-
• acute intoxication and addicted doctors
-
• drink driving
-
• self-harm and brief intervention
-
• detoxification
-
• delirium tremens and Wernicke's and Korsakoff's syndromes
-
• hepatitis
-
• portal hypertension and liver transplantation
-
• cardiac effects
-
• pathological jealousy.
This scale of project was made possible by Edinburgh's pioneers in the field, who have developed authoring software to assist translating content into an interactive format.
Progress has been slow largely because of competing priorities for clinicians and also technicians. However, the two latest modules have been written by three medical students as selected study components and summer projects. Plans to match the story lines with the appearance of topics in the curriculum have been complicated by course reorganisation. Nevertheless, in the 5 years since the project's inception, nine modules have been completed and a further two are well into development. Much time has been invested but the finished products have tended to restore faith in multi-disciplinary working. For example, we have developed an interactive drinking diary that generates feedback on the health risks of different patterns of drinking, and a diagram of the brain that changes colour when the student selects the correct anatomical area responsible for the various symptoms of intoxication (Figs. 1 and 2).
Evaluation
Novel educational interventions can be evaluated with as much or as little rigour as new treatments or service developments (Reference MorrisonMorrison, 2003). Evaluation is essential as part of the production process and ideally should be undertaken in the longer term to establish the cost-effectiveness of the work. Authors can view an anonymised list of all answers submitted, which can help to identify ambiguous questions. Our students are given ‘marks’ as they progress through the module, but this does not count towards their final course mark. The computerised nature of online learning can give information about when, by whom and for how long these programmes are accessed. In the 8 weeks after the formal launch of the first two modules in the second year of the undergraduate course, 60% of the students accessed the material and spent a median time of 25 min on each visit. Evaluation of an earlier Edinburgh series of online learning modules on the respiratory system suggests that although textbooks and own notes remain popular, computer packages are particularly valued as revision tools and the students who work through the material for reasons other than revision are also the high achievers (P. Warren, personal communication).
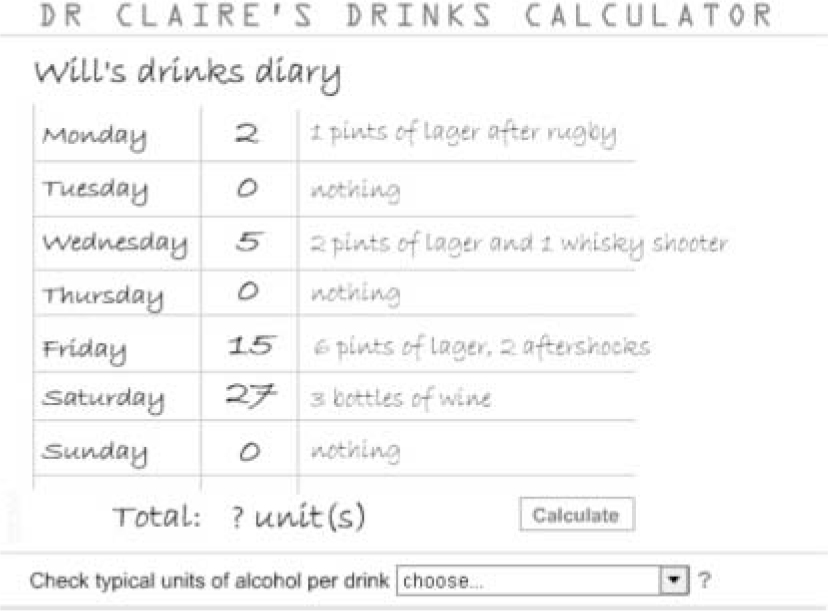
Fig. 1. An example of a computer-assisted learning module: an interactive drinking diary.
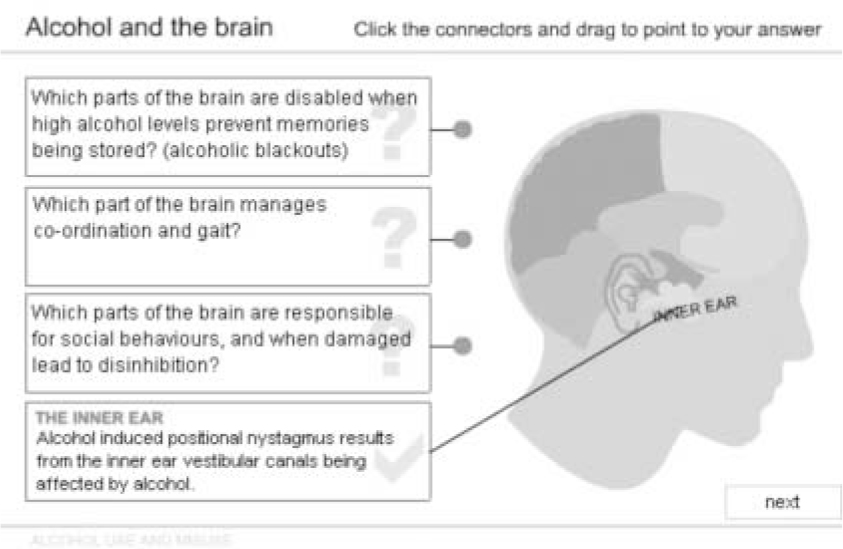
Fig. 2. An example from a computer-assisted learning module on the effects of alcohol on the brain.
Conclusion
Even the best computer simulations will never substitute for the experience of seeing real patients or for traditional textbooks, but they can nevertheless form an engaging learning experience in psychiatry. They can be deployed throughout psychiatric education and can assist in integrating psychiatric teaching with that of other medical specialties. Computer-delivered modules are popular with students, and although time-consuming to produce, they can be repeated as often as the student requires.
Future plans
Presentation of our project at the 2005 summer meeting of the Scottish Division of the College has opened up discussions on sharing the modules with all Scottish medical schools through the Scottish Deans’ Group. This may provide an opportunity for evaluating the series as a whole. Similar techniques are equally applicable to post-graduate education; the Royal College of Psychiatrists is developing online materials for psychiatrists to use for their continuing professional development and is actively recruiting potential authors and reviewers. Anyone interested in contributing should look on the College CPD online website at http://www.psychiatrycpd.org.
Declaration of interest
None.
Acknowledgements
We thank Dr Sandy Reid, the pathologist who pioneered online learning at the University of Edinburgh and Ms Mary Hutchison and Jackie Aim, the technicians who designed and developed the programme graphics, through Edinburgh's Learning Technology Organisation.



 Open access
Open access
eLetters
No eLetters have been published for this article.