


There has been has a long history of migration in Germany since the 17th century. Early, many Germans immigrated to Russia. During World War II their offspring settled in Siberia and Kazakhstan. Meanwhile many of them returned to Germany. In the 1950s, a large group of foreign workers from Southern Europe immigrated and were consequentially followed by their families. In the 1990s, migration streams were modified by the ‘fall of the iron curtain’ and the civil war in the former Yugoslavia, bringing re-settlers from the Eastern Bloc and refugees to Germany. Hence, the migrant population in Germany is a heterogeneous group, with a majority coming from Turkey and the former Soviet Union. Currently, more than 7 million foreigners (9 % of the population) and about 12 million Germans with a migration background (10 % of the population) live in Germany, which results in a rate of 19 % of the overall population(1).
Health-related risks and health behaviour are affected by cultural influences. Important aspects of dietary habits develop very early in life and mostly persist until adulthood(Reference Birch and Fischer2, Reference Leach3). Sustainable changes in life, for example migration, can influence these dietary patterns. However, little is known about the dietary habits of migrants, in particular among children and adolescents. Previous studies show several changes in eating habits after migration, but in different directions. Some investigators determined healthier dietary patterns among migrants(Reference Gedrich and Karg4, Reference Darmon and Khlat5), others in the local population(Reference Bau, Matteucci Gothe and Borde6). Data among migrants in The Netherlands showed for example that children from Morocco and Turkey ate fish and rice or pasta more often, and meat and soft drinks less often, than Dutch children. Furthermore, Turkish/Moroccan children skipped breakfast more often than children of Dutch origin(Reference Brussaard, van Erp-Baart, Brants, Hulshof and Löwik7). As shown in a recent twin study, even migration from Finland to Sweden was significantly associated with changes in dietary pattern(Reference Hammar, Hakala, Jorgensen, Becker, Hedlund, Ronnemaa, Koskenvuo and Kaprio8). The aim of the present study was to determine the specific food intake of children and adolescents living in Germany with different migrant status from a representative sample.
Methods
In KiGGS (German Health Interview and Examination Survey for Children and Adolescents), nationwide representative data of 17 641 children and adolescents aged 0 to 17 years were collected between May 2003 and May 2006 in 167 sample points. The sample was drawn in a two-stage procedure. In the first step, sample points were randomly selected with regard to federal state and community size. In these points, random samples of participants were selected stratified by age. The study design and methods have been described in detail elsewhere(Reference Kurth, Kamtsiuris and Hoelling9). All participants were interviewed and investigated comprehensively about their health, health behaviour and sociodemographic characteristics. All parents and participants aged 11 years or older were asked to fill in a self-administered questionnaire on health-relevant topics. This questionnaire exists in different versions related to the age of participants and was available in seven different languages (German, Turkish, Russian, Serbo-Croatian, Arabic, English and Vietnamese). Questions were also asked about nationality, country of birth, year of immigration (of the parents) and language spoken. Furthermore, medical examinations and medical history interviews were conducted by trained medical staff. The survey was approved by the Federal Office for Data Protection and the ethics committee of Charité University of Medicine, Berlin. All parents provided written informed consent. The overall response rate was 66·6 %.
A two-sided migration background was assumed using information on nationality, country of birth and language spoken at home under the following conditions: the participants themselves immigrated to Germany; both parents were not born in Germany; or both parents immigrated to Germany or had no German nationality(Reference Schenk, Ellert and Neuhauser10). For the presented analyses we grouped them into Turkish, Russian Germans (immigrants of German origin from the former Soviet Union), other migrants (other than Turkish or Russian Germans) and non-migrants. Information on parents’ income, occupational status and education was used to quantify socio-economic status (SES), which was categorised into low, medium and high(Reference Lange, Kamtsiuris, Lange, Schaffrath Rosario, Stolzenberg and Lampert11). The participants’ main residence was assessed and categorised into former West or East Germany. The degree of urbanisation was grouped into five categories: rural (under 5000 inhabitants), small town (from 5000 to under 20 000 inhabitants), middle-sized town (from 20 000 to under 100 000 inhabitants) and urban (100 000 or more inhabitants).
A retrospective semi-quantitative FFQ was used to assess dietary habits(Reference Mensink and Burger12). Two versions of this FFQ (identical in content) exist: one to be filled in by parents of 1- to 10-year-olds and the other to be filled in by the participants aged 11 to 17 years. This questionnaire was available only in German language. The FFQ covered the food frequencies and average portion sizes of forty-five foods in the last few weeks. Answer categories for the frequency questions were identical for all food items: never, once/month, 2–3 times/month, 1–2 times/week, 3–4 times/week, 5–6 times/week, once/d, 2–3 times/d, 4–5 times/d, >5 times/d. Portion sizes were divided into five categories; for example, 1/4 portion (or less), 1/2 portion, 1 portion, 2 portions, 3 portions (or more). To standardise the estimation of portion sizes, most were illustrated with pictures. Missing values in the FFQ were handled as follows. If the food frequency was available but portion size was not (n 1289), the middle category of portion size (usually one portion) was imputed. If both the food frequency and the portion size were missing (n 1588), the food item was considered to be not consumed (zero). If no food frequency but a portion size was given (n 66), the food item was considered a missing value. To calculate average food intake, frequencies were recoded into times of servings per month (where 1 month was set equal to 4 weeks); for example, never = 0, once/d = 28, >5 times/d = 168. For frequency bands such as 1–2 times/d the arithmetic mean was used (1·5). Finally, daily food intake was calculated by multiplication of food frequency and portion size.
Dietary score
For an overall interpretation of the diet quality of the participants, a dietary scored based on the FFQ items was constructed and is described in detail elsewhere(Reference Kleiser, Mensink, Scheidt-Nave and Kurth13). In brief, average food intake of eleven food groups (beverages, fruit, vegetables, bread/cereals, pasta/rice/potatoes, milk/dairy products, eggs, meat/sausage, fish, butter/margarine, sweets/snacks/sugared drinks) was compared with age- and sex-specific food-based dietary guidelines for children and adolescents(Reference Kersting, Alexy and Clausen14) by calculating the ratio (food intake divided by recommended intake). Depending on the guidelines to eat plenty, moderate or small amounts of specific foods, each of these food ratios was then allocated with points ranging from zero to 100 for every food group. For each food group maximum points were given when the recommendation was totally met. Finally, these single scores were added together and standardised to a total scale from zero to 100. A higher score value implies a better overall dietary quality.
Statistical analyses
Statistical analyses refer to children and adolescents aged 3 to 17 years for whom complete data on food intake were available (7186 boys and 6919 girls). For descriptive analyses and comparison of migrant groups, prevalence, means and 95 % confidence intervals were calculated. Finally, a stepwise linear regression model was used to analyse associations between migration background and health quality of the diet. Since the sample is based on a clustered and stratified design, all analyses were performed with complex sample procedures in the SPSS statistical software package version 14·0 (SPSS Inc., Chicago, IL, USA). To enhance the representativeness of the sample, a weighting factor was used in the analyses which corrects for the deviances of the net sample to the population structure (at 31 December 2004) concerning age, gender, residence (West Germany, East Germany, Berlin) and nationality(Reference Kamtsiuris, Lange and Schaffrath Rosario15). All tests were performed two-sided and P values less than 0·05 or non-overlapping confidence intervals were considered to be statistically significant.
Results
Study population
From the 17 641 children and adolescents participating in KiGGS, 2590 (17·1 %, weighted) had a (two-parent) migration background. In the total KiGGS sample, 726 (4·8 %, weighted) of participants were of Turkish origin, 518 (3·5 %, weighted) Russian Germans (immigrants of German origin from the former Soviet Union) and 1346 (8·8 %, weighted) were of other origin (other than Turkish or Russian German). The largest proportion of migrants was Turkish with 28·2 %, followed by Russian Germans with 20·4 %. Participants with a migration background more often had low SES compared with non-migrant participants (53·7 % v. 22·6 %). Turkish boys and girls showed the highest proportion of low SES with 74·7 %. The overall response rate was 66·6 %.
The overall response for the FFQ was 95·4 %. A completed FFQ was available for 97·4 % of non-migrants, 90·1 % of Russian Germans, 83·9 % of other migrants and 76·8 % of Turkish migrants.
There were no statistically significant differences between responders and non-responders according to age group and BMI among the different migrant groups. Among Turkish migrants only, more boys than girls completed the FFQ. However, more Turkish boys than Turkish girls were present in the analysed data set. Among all migrant groups and non-migrants, the proportion of non-responders was higher for participants with low SES compared with those with higher SES (data not shown).
Dietary behaviour
Table 1 shows the average food intake in grams per day stratified by migrant group. Turkish children and adolescents consumed significantly more soft drinks, tap water, cereals/cornflakes, white bread/rolls, cream cheese, soup, (deep-) fried potatoes, chocolate cream and snacks than all other groups. Furthermore, Turkish participants ate significantly less meat (without poultry and sausage/bacon) than other migrants and non-migrants. Non-migrants ate significantly less fruit, biscuits and chocolate and more frozen vegetables compared with all other groups. Several differences occurred between Turkish migrants and non-migrants. Turkish children and adolescents ate significantly more cheese, sweets and pudding/rice pudding and drank significantly less milk than non-migrants. Migrants from Turkey and other migrants ate more poultry, fish and pasta/rice, and less sausage/bacon and cooked potatoes, than migrants from Russia and non-migrants. Turkish children and adolescents consumed significantly more eggs and fast food than Russian Germans and non-migrants, and other migrants consumed more of those food groups than non-migrants. Other migrants and non-migrants ate significantly more cooked vegetables (prepared from fresh vegetables) than participants from Russia. The consumption of vegetables in total (including salad) showed a tendency to a higher consumption in Turkish and non-migrants compared with participants from Russia (not significant). Consumption of vegetables without salad was significantly higher in non-migrants than in Russian Germans. No statistically significant differences were shown in consumption of mineral water, wholegrain bread, preserved fruit, raw vegetables/salad and cake/pastry.
Table 1 Average food intake (g/d) by migrant group: young migrants (children and adolescents aged 3 to 17 years) living in Germany, 2003–6

Significant differences between migrant groups (non-overlapping confidence intervals) are highlighted (bold).
*Fried sausage, curry sausage, hamburger, doner kebab.
Table 2 shows the key values of the dietary score. The score values showed a normal distribution. The weighted mean value of the score was 55 with a minimum of 19 and a maximum of 94 points. Ten per cent of the children and adolescents had a score value below 41 and another 10 % above 69. The mean values of this score according to migrant groups are presented in Fig. 1. It showed a 3·3 point higher (better) value for non-migrants compared with Russian German children and adolescents. This difference was statistically significant. The dietary score of non-migrants was also significantly higher than that of other migrants. The small confidence interval of non-migrants resulted from the higher number of cases.
Table 2 Main characteristics of the dietary score: young migrants (children and adolescents aged 3 to 17 years) living in Germany, 2003–6


Fig. 1 Dietary score by migrant group: young migrants (children and adolescents aged 3 to 17 years) living in Germany, 2003–6. Values are means with their 95 % confidence intervals represented by vertical bars
Figure 2 shows the mean values of the dietary score according to age group and sex. In every ethnic group younger boys and girls showed a better score, on average, than their older counterparts. Girls had a better mean score than boys of the same age, except the 11- to 17-year-old Turkish and Russian German migrants. However, these differences were not often statistically significant. Only younger boys from Turkey had a significantly lower (worse) score than non-migrants boys of the same age. Russian German girls aged 11 to 17 years had a significantly lower mean score than similarly aged non-migrant girls. In general, Turkish and Russian German children and adolescents showed a worse score than other migrants and non-migrants (Fig. 2).

Fig. 2 Dietary score by age group, sex and migrant group (![]() , Turkish migrants;
, Turkish migrants; ![]() , Russian German migrants;
, Russian German migrants; ![]() , other migrants;
, other migrants; ![]() , non-migrants): young migrants (children and adolescents aged 3 to 17 years) living in Germany, 2003–6. Values are means with their 95 % confidence intervals represented by vertical bars
, non-migrants): young migrants (children and adolescents aged 3 to 17 years) living in Germany, 2003–6. Values are means with their 95 % confidence intervals represented by vertical bars
Finally, a stepwise linear regression model was developed with dietary score as the dependent variable (Table 3). If only age, sex and migrant group were considered in the model (model 1), all migrant groups showed a significant association with dietary quality. When additionally SES was included (model 2), only the association with Russian German participants remained statistically significant. The possibility of a less favourable diet was therefore higher with increasing age, for boys, Russian Germans and participants with a low SES. Living in rural areas, small or middle towns was also associated with a less favourable diet (model 3).
Table 3 Determinants of the dietary score (linear regression models): young migrants (children and adolescents aged 3 to 17 years) living in Germany, 2003–6
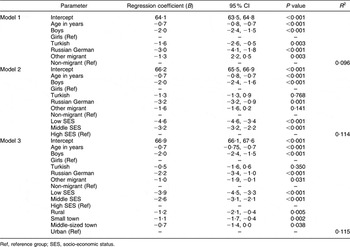
Ref, reference group; SES, socio-economic status.
Discussion
The analyses of daily food intake indicate considerable migration-specific differences in dietary habits. Overall, Turkish and Russian German migrants showed a less favourable diet compared with non-migrants although some aspects of their eating habits were preferable, for example the higher fruit consumption. On the other hand, Turkish children and adolescents consumed the highest average amounts of soft drinks, white bread and rolls, fried potatoes or potatoes chips, chocolate and snacks. Participants from Russia consumed the lowest amounts of beverages and vegetables (but similar amounts of fruit as the Turkish) and ate the highest amounts of sausage or bacon. Non-migrants consumed the lowest amounts of biscuits, chocolate, sweets and snacks. The healthy diet score, which is based on a comparison with the current recommendation, was lowest for Russian Germans. Furthermore, participants with low SES had a lower dietary score. Since children and adolescents with a migration background were disproportionally often participants with low SES, we adjusted for SES in our analyses. After adjusting for SES, the association between the dietary score and migration background changed. For example, there was no longer a significant association among Turkish migrants. SES is independently associated with food intake, which may explain part of the association between food intake and migration background. However, in the multiple linear regression models a migrant-specific association with overall diet quality remained, independent of SES.
The results of our study are in line with several former investigations which determined differences in eating habits between migrants and non-migrants(Reference Hammar, Hakala, Jorgensen, Becker, Hedlund, Ronnemaa, Koskenvuo and Kaprio8, Reference Landman and Cruickshank16). However, lifestyle and nutrition are influenced by many factors, such as degree of integration, duration of stay, generation of migration and language ability(Reference Darmon and Khlat5, Reference Pan, Dixon, Himburg and Huffman17, Reference Lee, Sobal and Frongillo18). Some researchers conclude that migrants better meet national recommendations than natives(Reference Darmon and Khlat5, Reference Brussaard, van Erp-Baart, Brants, Hulshof and Löwik7). For example, the average macronutrient intake of migrant children from Surinam and Mediterranean areas, as well as of Turkish and Moroccan women, was more in line with the Dutch dietary guidelines than the traditional Dutch diet(Reference Brussaard, van Erp-Baart, Brants, Hulshof and Löwik7). Furthermore, North African migrant men living in France had a better overall diet quality than natives(Reference Méjean, Traissac, Eymard-Duvernay, El Ati, Delpeuch and Maire19). However, in our analyses migrant children and adolescents, especially Russian Germans and Turkish, were not more likely to eat according to the national recommendation than non-migrants. It seems that migrant children and adolescents have more strongly adapted less preferable aspects of the modern Western diet; for example, indicated by the high consumption of soft drinks, fast food and sweets among Turkish migrants.
Differences in the results of studies focusing on dietary behaviour among migrants may not only strongly reflect the differences in the initial food culture of the major migrant groups, but also the differences in the traditional food culture of the resident countries. Migrant groups differ historically between different countries. For instance, Turkish people are a major migrant group in Germany, whereas in France a large proportion of migrants are African. Therefore, a cross-national comparison is difficult. Next to the cultural differences, differences in national food guidelines and evaluation tools make comparisons of results complicated. For instance, our dietary score is strongly based on national recommendations and is a relatively subjective instrument.
The strengths of our study include the large sample size and national representativeness across a wide age range, its good response rate for migrants and non-migrants, and the detailed information on the migration background and on food habits. In KiGGS specific effort was made in the study design to adequately integrate persons with a migration background. For example, the main questionnaires were available in seven different languages(Reference Schenk, Ellert and Neuhauser10). The proportion of migrants of 17 % in the study population reflects a good representativeness of the overall migrant population living in Germany (currently 19 %). However, our study does not claim to be representative for all migrant groups. Furthermore, the FFQ exists in German only and contains a limited number of items. It may be that some items in the FFQ are less sensitive for the special food habits of migrants. More open-ended instruments such as food records or 24 h recalls may be more culture-specific. However, the food groups in the FFQ are relatively broad so it may be assumed that, on this rough level, it may assess intake in a standardised and comparable way. Probably since the FFQ was not translated, a lower completion rate was seen among migrants in comparison to non-migrants. Furthermore, there was an overall lower response for children and adolescents with low SES. Although we adjusted for SES in the multivariable analysis, this could result in an underestimation of differences between migrants and non-migrants.
In conclusion, our results suggest that there are several differences in the dietary habits of children and adolescents with different migration background. This finding is of public health relevance since migrant children are not only a large but also a vulnerable population group. Furthermore, their lower SES interrelates not only with their nutrition but also with other health-related factors. Since dietary habits formed in childhood are often preserved throughout life and are of importance for a variety of lifestyle-related diseases, positive dietary habits need to be recognised and strengthened while unhealthy diets need to be prevented as early as possible. A nutritionally valuable diet with plenty of fruit, vegetables and carbohydrate-rich foods is an important health-promoting resource and should be strengthened. The disadvantages of supposed modern Western nutrition should be highlighted and made a subject of discussion. There is a need to set special focus points in promoting of healthy dietary behaviour among children and adolescents with a migration background.
Acknowledgements
KiGGS was funded by the German Federal Ministry of Health, the German Federal Ministry of Education and Research, and the Robert Koch Institute. The present analyses were supported by the German Federal Ministry of Food, Agriculture and Consumer Protection. None of the authors had any conflict of interest. All authors contributed to interpretation of the data and revision of the manuscript.





