



More than 50 years have passed since epidemiological observations suggested that processing grains with the removal of varying proportions of the bran and germ, including dietary fibre, may play a part in development of cardiometabolic diseases(Reference Cummings and Engineer1,Reference Reynolds, Akerman and Mann2) . Despite the well-established health benefits, little has been achieved concerning the global intake of whole-grain foods since then, which remains substantially lower than recommended levels(Reference Mann, Pearce and Seal3–5). In 2017, low intake of whole grains was among the leading dietary risk factors identified for death and disability-adjusted life-years worldwide, accounting for 3 million deaths and 82 million disability-adjusted life-years(5). At the same time, grain foods are still the major carbohydrate-providing foods in the global diet, also contributing to protein, fibre and micronutrient intake (according to the degree of processing) in many populations(6,Reference Seal, Nugent and Tee7) . This central role in the human diet makes them a convenient target for nutrition policies focused on improving dietary quality and reducing disease burden(Reference Mattei, Malik and Wedick8). In Brazil, for example, there is mandatory fortification of maize and wheat flour with Fe and folic acid, but there is no information regarding fortification of grain products with other nutrients on a population basis(9).
Owing to challenges of intervention studies, such as sufficient sample size, duration, participant adherence and economic feasibility, dietary modelling studies are becoming more frequent as they enable comparisons between hypothetical scenarios and can provide evidence which can then be tested in targeted interventions and converted into policies(Reference Grieger, Johnson and Wycherley10). In this context, modelling studies that estimate the impact of dietary strategies to increase consumption of more healthful grain foods are essential to inform evidence-based policy actions. Prior investigations focusing on changing from refined to whole-grain consumption reported improvements in dietary nutrient density and quality, and even a reduction in diet cost(Reference Keast, Rosen and Arndt11–Reference Mann, Yu and Hopkins14). However, these studies were developed in high-income countries, and generalisability of findings to low- and middle-income countries is limited due to differences in dietary intake of carbohydrate-rich foods, upon which the modelling strategy is based(Reference Dehghan, Mente and Zhang15). Additionally, varying strategies can be used to achieve the goal of the modelling process, which are usually culturally specific.
To our knowledge, approaches to increase the intake of more healthful grain foods in Brazil have not been previously tested. This information may provide a useful overview for subsequent interventions, given the importance of grains in the Brazilian diet and the high disease burden associated with low whole-grain intake in the country(5). The present study aimed to estimate the potential nutritional impact of replacing staple grain foods with more healthful grain food options in the population of São Paulo, Brazil, under current eating patterns. We hypothesised that the substitution of white rice and white bread, which are among the five most consumed foods in the country(Reference Souza, Pereira and Yokoo16), by equivalent more healthful options (brown rice and whole-wheat bread) would result in improvement in diet nutritional content.
Methods and materials
Data source
Data came from the 2015 Health Survey of São Paulo (Inquérito de Saúde de São Paulo), the third edition of a complex, multistage probability, cross-sectional survey designed to represent São Paulo urban residents(Reference Alves, Escuder and Goldbaum17). The municipality is one of the world’s most populous cities (more than 12·3 million people lived in São Paulo in 2020), located in south-eastern Brazil. The survey included 4059 participants aged over 12 years (865 aged 12 to 19 years, 2169 aged 20 to 59 years and 1025 aged over 60 years) that completed a semi-structured questionnaire regarding demographic and socio-economic data, as well as lifestyle information(Reference Alves, Escuder and Goldbaum17). A subsample of 1741 participants (553 aged 12 to 19 years, 643 aged 20 to 59 years and 545 aged 60 years or more) completed a 24-h dietary recall, on which the substitution models in the current study were based. Further information regarding the study design is described by Fisberg et al. (Reference Fisberg, Sales and Fontanelli18).
Dietary intake data were collected during the household interview using the Multiple Pass Method(Reference Moshfegh, Rhodes and Baer19). Self-reported foods and beverages consumed were converted into nutritional values using the Nutrition Data System for Research software 2014 version (Nutrition Coordinating Center, University of Minnesota). Nutrient content of food items included in the survey was compared with those available in Brazilian national food composition tables(20,21) . Nutritional values in the database were corrected if the concordance rate was not between 80 % and 120 % with corresponding foods consumed by the São Paulo population(Reference Fisberg, Sales and Fontanelli18).
Socio-demographic variables
Demographic and socio-economic data were assessed using a standardised questionnaire collected during face-to-face interviews. Participants were categorised in the following age groups: 12 to 19 years, 20 to 59 years and over 60 years, according to the definitions of the WHO and the Brazilian Statute for Children and Adolescents(22,23) . Education level was categorised as below high school graduate, high school graduate/equivalent and college or some college. Individual education was considered for adults, and householder education was used for adolescents. Per capita family income was calculated as the sum of the income of all family members and divided by the number of family members and was considered as less than one minimum wage, two to three minimum wages, more than three minimum wages and ‘do not know’. The monthly minimum wage was 788·00 Brazilian Reals (BRL) in 2015, equivalent to 253·00 United States Dollars (USD) (currency exchange based on the Brazilian Central Bank on 1 July 2015). Self-reported ethnicity classification was based on Brazilian law for admission into public universities (number 12711) as ‘white or yellow’ and ‘black, brown or indigenous’(24). This is an affirmative law that determines the number of public university vacancies that should be fulfilled by self-declared black, brown or indigenous populations(Reference Santos, Souza and Sasaki25).
Substitutions models
The main feature of the current study was the systematic replacement of white rice and white bread reported as consumed in the 24-h dietary recall with brown rice and whole-wheat bread, respectively. Food items were selected based on the top ten contributors to energy intake from grain foods estimated in a previous investigation performed with the same population(Reference Fontanelli, Micha and Sales26). White rice and white bread (French bread and commercial white bread) accounted for 57·0 % of energy intake from grain foods not containing 1 g of fibre per 10 g of carbohydrate (not meeting the carbohydrate to fibre ≤ 10:1-ratio), which was used as a criterion to identify more healthful grain foods(Reference Fontanelli, Micha and Sales26). Three approaches were then used to replace each food item by its nearest more healthful grain food equivalent: model (1) white rice was replaced with brown rice; model (2) white bread was replaced with whole-wheat bread; model (3) white rice was replaced with brown rice, and white bread was replaced with whole-wheat bread, i.e. model 1 plus model 2 (see online supplementary material, Supplemental Table 1). The amount (in grams) of the original food item was replaced by the same amount of the alternative product. Nutritional values of food items included in the substitution models are shown in see online supplementary material, Supplemental Table 2.
The consequences of the substitution models on nutrient and energy intakes were estimated considering whether 25 %, 50 %, 75 % or 100 % of the population had their consumption changed. Assuming that complete replacement models are not achievable from a public health perspective, partial substitution models better represent the probable impact of corresponding interventions. Participants were assigned into subsamples (25, 50 and 75 %) by creating a uniformly distributed random variate over the interval (0,1). The proportion of socio-demographic characteristics and rice or bread consumption was similar comparing subsamples to the total sample (see online supplementary material, Supplemental Table 3). For participants consuming white rice or white bread more than one time per day, we also estimated the potential nutritional impact of replacing white rice and white bread in one eating occasion, with the purpose to explore if a one-time replacement is enough to provide significant changes in the population’s diet. Substitution models were also performed for sex and age subgroups to investigate possible differences among replacement models.
Statistical analyses
The association between the prevalence of consumers of grain foods included in the modelling process and demographic and socio-economic characteristics was assessed using χ 2 tests. White rice consumers, white bread consumers and those consuming either white rice or white bread represent the part of the population that had their consumption changed in the replacement models 1, 2 and 3, respectively.
Study primary outcomes included change in observed intake of more healthful grain foods (foods meeting the carbohydrate to fibre ≤ 10:1-ratio, g/d) and the contribution of more healthful grain foods to total grains (%). We considered as secondary outcomes the percent change of energy (kcal/d) and the following nutrients: carbohydrate (g/d), available carbohydrate [carbohydrate – dietary fibre] (g/d), dietary fibre (g/d), total sugar (g/d), added sugars (g/d), protein (g/d), total fat (g/d), SFA (g/d), PUFA (g/d), MUFA (g/d), vitamin B1 (mg/d), vitamin B2 (mg/d), vitamin B3 (mg/d), vitamin B6 (mg/serving), folate (DFE µg/d), vitamin E (mg/d), Na (mg/d), Ca (mg/d), K (mg/d), iron (mg/d), Se (µg/d), Mg (mg/d) and Zn (mg/d). All study participants were included in the modelling process, but only participants reporting white rice or white bread intake had their consumption changed.
Changes in intakes of more healthful grain foods, energy and nutrients were tested for significance using t-tests. Given the large number of participants consuming the refined versions of bread and rice, and as a result affected by the substitution models, even small differences between observed and modelled intakes would be statistically significant. For that reason, statistically significant changes were only interpreted if relative change in intake was 5 % or more comparing pre and post-modelled intake (considered ‘moderate’ changes), and statistically significant changes in intake greater than 10 % (or less than –10 %) were described as ‘strong’. These cut-off points were used in a previous study, which adopted a 10 % value based on the definition of the United States Food and Drug Administration of a ‘good source’ of nutrients(Reference Rehm and Drewnowski13,27) . As this value varies according to the nutrient in question in the Brazilian legislation, we opted to use the United States Food and Drug Administration cut-off point(28).
Stata version 14.0 (StataCorp) was used to perform the modelling process, and statistical significance was established at two-sided P < 0·05. We used the survey module of Stata to account for the complex survey sampling design of the study, and as a result, findings from the current study are considered representative of the São Paulo population aged 12 years or more.
Results
The majority of the population consumed white rice (80·8 %), white bread (62·8 %) and ate either white rice or white bread (91·6 %) on the assessment day, but brown rice, whole-wheat bread or either brown rice or whole-wheat bread consumption was limited, 3·3, 4·6 and 7·5 %, respectively (Table 1). Higher prevalence of white rice consumers was observed among males, those with education level below high school graduate, with family income per capita between one and three minimum wages, and those who self-reported black, brown or indigenous ethnicity. For brown rice, higher prevalence of consumption was observed among females. Higher prevalence of white bread consumption was observed among males, and those with education level below high school graduate. For whole-wheat bread, higher prevalence of consumption was observed among participants aged 60 years or more, females, those with education level of college or some college, with family income per capita more than three minimum wages, and who self-reported white or yellow ethnicity. Considering participants who consumed either white rice or white bread, higher prevalence of consumption was observed among males, those with education level below high school graduate, and family income per capita lower than one minimum wage, and those who self-reported black, brown or indigenous ethnicity. On the other hand, higher prevalence of either brown rice or whole-wheat bread consumption was observed among participants aged 60 years or more, females, those with college and some college education, with family income per capita more than three minimum wages, and those who self-reported white or yellow ethnicity.
Table 1 Consumption of rice and bread by socio-demographic characteristics among São Paulo population aged 12 years or older based on the 2015 Health Survey of São Paulo

*P-value < 0·05; **P-value < 0·01; ***P-value < 0·001 in survey weighted χ 2 tests for prevalence of consumers v. prevalence of nonconsumers.
† Minimum wage was BRL 788·00 (equivalent to USD 253·00) in 2015.
‡ Participants who reported the intake of white rice or brown rice in the 24-h dietary recall.
§ Participants who reported the intake of white bread or whole-wheat bread in the 24-h dietary recall.
The pre-modelled and post-modelled population daily consumption of more healthful grain foods, energy and nutrient intakes are reported in Tables 2, 3 and 4 and Figs 1 and 2. All white rice consumed by São Paulo population was replaced with brown rice in model 1 at 100 % change. This resulted in moderate percent changes among available carbohydrate (–5·4 %, 95 % CI: –5·8, –5·1), and strong percent changes were found for vitamin B1 (–10·9 %, 95 % CI: –11·5, –10·2), dietary fibre (18·0 %, 95 % CI: 16·9, 19·1) and Mg (45·0 %, 95 % CI: 41·8, 48·1) (Fig. 1). After the replacement of all the white bread consumed for whole-wheat bread (model 2 at 100 % change), moderate percent changes were observed for Zn (5·6 %, 95 % CI: 5·2, 6·1), folate (–7·8, 95 % CI: –8·3, –7·3), Mg (8·0 %, 95 % CI: 7·4, 8·5), Fe (–8·1 %, 95 % CI: –8·6, –7·7), dietary fibre (9·0 %, 95 % CI: 8·3, 9·6), Ca (9·4 %, 95 % CI: 8·5, 10·3) and vitamin B1 (–9·9 %, 95 % CI: –10·6, –9·1), while strong changes were found for vitamin B6 (–12·5 %, 95 % CI: –13·4, –11·6), vitamin E (14·5 %, 95 % CI: 13·4, 15·7) and vitamin B2 (–17·3 %, 95 % CI: –18·5, –16·1) (Fig. 1). The substitution of all white rice and white bread for brown rice and whole wheat bread, respectively (model 3 at 100 % change) resulted in moderate percent changes for total carbohydrate (–6·1 %, 95 % CI: –6·4, –5·8), folate (–6·6 %, 95 % CI: –7·1, –6·1), available carbohydrate (–8·5 %, 95 % CI: –8·9, –8·1), Fe (–8·6 %, 95 % CI: –9·1, –8·1), Zn (9·1 %, 95 % CI: 8·6, 9·6) and Ca (9·3 %, 95 % CI: 8·4, 10·2), while strong changes were observed for vitamin B6 (–12·5 %, 95 % CI: –13·4, –11·6), vitamin B2 (–17·4 %, 95 % CI: –18·6, –16·2), vitamin E (18·8 %, 95 % CI: 17·5, 20·1), vitamin B1 (–20·7 %, 95 % CI: –21·8, –19·7), dietary fibre (27·0 %, 95 % CI: 25·6, 28·3) and Mg (52·9 %, 95 % CI: 49·6, 56·3) (Fig. 1).
Table 2 Estimated survey-weighted mean energy and nutrient intake after replacing white rice for brown rice (model 1) on a proportional basis among São Paulo population aged over 12 years based on the 2015 health survey of São Paulo

DFE, dietary folate equivalents.
Asterisks indicate statistical significance comparing whether modelled changes are 5 % change or more from observed intakes. *P-value < 0·05; **P-value < 0·01; ***P-value < 0·001 in survey weighted t tests.
† Values represent total daily energy and nutrients consumed by São Paulo residents (n 1741).
‡ Proportion of the population that had their white rice consumption replaced by brown rice.
§ Observed v. 100 % change.
Table 3 Estimated survey-weighted mean energy and nutrient intake after replacing white bread for whole-wheat bread (model 2) on a proportional basis among São Paulo population aged over 12 years based on the 2015 health survey of São Paulo
DFE, dietary folate equivalents
Asterisks indicate statistical significance comparing whether modelled changes are 5 % change or more from observed intakes. *P-value < 0·05; **P-value < 0·01; ***P-value < 0·001 in survey weighted t tests.
† Values represent total daily energy and nutrients consumed by São Paulo residents (n 1741).
‡ Proportion of the population that had their white bread consumption replaced by whole wheat bread.
§ Observed v. 100 % change.
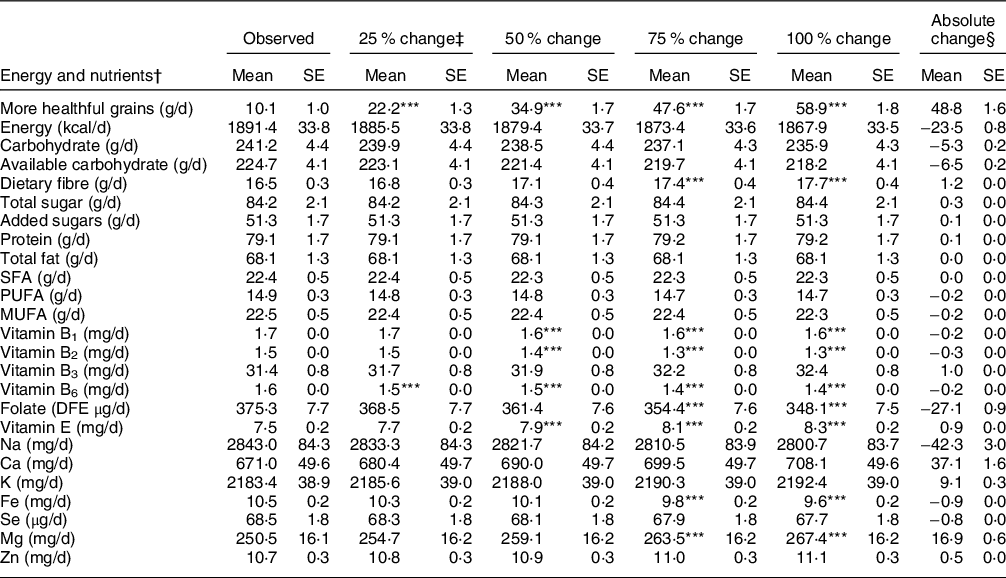
Table 4 Estimated survey-weighted mean energy and nutrient intake after replacing white rice for brown rice and white bread for whole-wheat bread (model 3) on a proportional basis among São Paulo population aged over 12 years based on the 2015 health survey of São Paulo

DFE, dietary folate equivalents.
Asterisks indicate statistical significance comparing whether modelled changes are 5 % change or more from observed intakes. *P-value < 0·05; **P-value < 0·01; ***P-value < 0·001 in survey weighted t Tests.
† Values represent total daily energy and nutrients consumed by São Paulo residents (n 1741).
‡ Proportion of the population that had their white rice consumption replaced by brown rice and white bread consumption replaced by whole wheat bread.
§ Observed v. 100 % change.

Fig. 1 Estimated survey weighted percent change in population mean intake of nutrients* per day according to substitution models based on the 2015 Healthy Survey of São Paulo. White bars represent the replacement of all white rice consumed by the population for brown rice (model 1). Light grey bars represent the substitution of all the white bread consumed by the population for whole-wheat bread (model 2). Dark grey bars represent the replacement of all white rice and white bread consumed by the population for brown rice and whole-wheat bread, respectively (model 3). Dashed grey lines represent the cut-off points for strong changes (10 % or –10 % change). Error bars represent se. *Only nutrients that changed more 5 % comparing observed and modelled intakes were presented.![]() Model 1: rice;
Model 1: rice;![]() Model 2: bread;
Model 2: bread;![]() Model 3: rice + bread.
Model 3: rice + bread.

Fig. 2 Estimated survey-weighted percentage of more healthful grain food intake from total grain foods intake in pre-modelled (observed) and post-modelled (replacement performed in 25 %, 50 %, 75 %, 100 % of the São Paulo population) according to substitution model: model (1) white rice replaced for brown rice; model (2) white bread was replaced for whole-wheat bread; model (3) white rice was replaced for brown rice, and white bread was replaced for whole-wheat bread, 2015 Healthy Survey of São Paulo. Bars represent se. Dashed grey lines represent the recommendation for whole grain to total grain intake.![]() Observed;
Observed;![]() 25 %;
25 %;![]() 50 %;
50 %;![]() 75 %;
75 %;![]() 100 %.
100 %.
In general, all replacement models resulted in an absolute increase of dietary fibre (from 1·2 g/d in model 2 to 4·0 g/d in model 3), in Mg intake (from 16·9 g/d in model 2 to 114·6 in model 3) and a decrease in vitamin B1 (from –0·3 mg/d in model 3 to –0·2 mg/d in models 1 and 2). Differences between models were observed for carbohydrate (–14·2 g/d in model 3), available carbohydrate (–11·8 g/d in model 1 and –18·3 g/d in model 3), vitamin B2 (–0·3 mg/d in models 2 and 3), vitamin B6 (–0·2 mg/d in models 2 and 3), folate (–27·1 µg/d in model 2 and –23·9 µg/d in model 3), vitamin E (+0·9 mg/d in model 2 and +1·1 mg/d in model 3), Fe (–0·9 mg/d in models 2 and 3) and Zn (+0·8mg/d in model 3) (Tables 2-4).
The majority of the modelling effects were seen if 100 % of the population had their consumption of white rice or white bread replaced with brown rice and whole-wheat bread. However, statistically significant changes were also observed at 25, 50 and 75 % substitution levels. At the 25 % level, Mg (models 1 and 3) and vitamin B6 (model 2) would change. At the 50 % level, changes would be seen for dietary fibre (models 1 and 3), vitamin B1 (models 1, 2 and 3), vitamin B2 (model 3), vitamin B6 (model 2), vitamin E (models 2 and 3) and Mg (models 1, 2 and 3). At the 75 % level, changes in available carbohydrate (model 3), dietary fibre (models 1, 2 and 3), vitamin B1 (models 1, 2 and 3), vitamin B2 (models 2 and 3), vitamin B6 (models 2 and 3), folate (model 2), vitamin E (models 2 and 3), Fe (models 2 and 3), Mg (models 1, 2 and 3) and Zn (model 3) would be observed.
Observed mean intake of more healthful grain foods before the models were applied was 10·1 g/d, and these foods were consumed by 15·8 % (95 % CI: 13·5, 18·3) of the population. Post-modelled absolute changes in more healthful grain foods consumption ranged from 48·8 g/d in model 2 to 220·2 g/d in model 3, both at the 100 % substitution level (Tables 3 and 4). At this level of intake, the majority of the population would be consuming at least one more healthful grain food, from 71·6 % of the population (95 % CI: 69·0, 74·0) in model 2 to 94·5 % of the population (95 % CI: 92·9, 95·7) in model 3. Pre-modelled intake of more healthful grain food as a percentage of total grains intake was 4·0 % (95 % CI: 3·3, 4·8) and increased to 52·5 % (95 % CI: 50·5, 54·5), 20·9 % (95 % CI: 19·6, 22·2) and 69·4 % (95 % CI: 67·3, 71·5) in models 1, 2 and 3, respectively (Fig. 2). Results from proportional substitutions indicate more healthful grain foods would increase significantly at 25, 50 and 75 % levels of population adherence (P < 0·001 for each level of substitution for each model, Tables 2-4).
Given that part of the population of São Paulo consumed either white rice or white bread more than one time a day (by 33·8 % of the population (95 % CI: 31·0, 36·7) for white rice and by 16·0 % of the population (95 % CI: 14·1, 18·0) for white bread), substitution models were also performed to estimate the replacement of these food items in one eating occasion and similar results were found, but the effects were smaller as expected (see online supplementary material, Supplemental Table 4). Changes in intake of nutrients by substitution models performed among age and sex subgroups were comparable to models performed considering the overall population, with the greatest impact among subgroups with lower prevalence of brown rice and whole-wheat bread consumption, such as adolescents and males (see online supplementary material, Supplemental Tables 5, 6, 7, 8, 9, and Figures 1 and 2).
Discussion
We estimated the potential nutritional impact of approaches to increase more healthful grain foods intake among São Paulo residents under current eating patterns. Substitution models were based on two staple grain foods, rice and bread, which together resulted in substantial changes on population dietary intake. Observed mean intake of more healthful grain foods before the substitutions was 10·1 g/d, which represented 4·0 % of total grain intake. This would potentially increase to 220·2 g/d, representing 69·4 % of total grain intake if the entire population currently consuming white rice and white bread changed all of their consumption to brown rice and whole wheat bread. Overall, estimated intakes of Zn, Ca, vitamin E, dietary fibre and Mg increased by more than 5 % after applying the models. In contrast intakes of total carbohydrate, available carbohydrate, folate, Fe and vitamins B6, B2 and B1 decreased by more than 5 % post-modelling. The results provide evidence for future interventions and policy efforts to improve the intake of more healthful grain foods.
Findings from the current study suggest that shifting consumption from usually eaten grain foods to more healthful equivalent options may represent a valuable strategy to increase the intake of nutrients with high prevalence of inadequacy among the Brazilian population (more than 70 %), such as dietary fibre, Mg, Ca and vitamin E(Reference Araujo, Bezerra and Barbosa29–Reference Souza, Barufaldi and Abreu34). It is interesting to note that the different modelling strategies led to different effects on the population nutritional intake. The substitution of white rice with brown rice resulted in greater changes in dietary fibre and Mg intake than occurred when substituting white bread with whole-wheat bread, while the replacement of white bread with whole-wheat bread produced greater changes in vitamin E and Ca dietary intake. As a result of the varied nutritional content and bioactive compounds in the food items, different physiological effects may be expected(Reference Bach Knudsen, Nørskov and Bolvig35,Reference Joye36) . Antidiabetic properties, decreased inflammation and the modulation of lipid metabolism and oxidative stress have been documented in in vitro studies and clinical trials investigating health benefits of consuming brown rice(Reference Mir, Shah and Bosco37). A recent systematic review and meta-analysis of randomised controlled trials found that, compared with white rice, brown rice led to an improvement in TAG levels (–1·6 mg/dl) in interventions ranging from 150 to 400 g of cooked rice(Reference Marshall, Petocz and Duve38). One serving of brown rice per day was also associated with reductions in type 2 diabetes risk (hazard ratio 0·72) in three large prospective studies from the USA; however, the association was no longer significant after adjusting for BMI(Reference Hu, Ding and Sampson39). For whole-wheat bread, there are also consistent beneficial effects reported. The intake of 90 g (∼3 servings) of whole-grain bread was associated with risk reductions of CHD (relative risk 0·83), CVD (relative risk 0·87), total cancer (relative risk 0·91) and all-cause mortality (relative risk 0·85)(Reference Aune, Keum and Giovannucci40). Dark bread consumption was also associated with type 2 diabetes risk reduction and significant effects were seen for just one serving of this food (hazard ratio 0·93 (95 % CI: 0·91, 0·95)(Reference Hu, Ding and Sampson39). Findings from an earlier study performed with the same population suggested that each 1 % increase in energy intake from more healthful grain foods (including brown rice and whole-wheat bread) was associated with lower concentrations of blood TAG (–10·7 %), reduced TAG/HDL cholesterol ratio (–14·9 %), fasting insulin (–13·6 %) and homoeostasis model assessment for insulin resistance (–14·0 %)(Reference Fontanelli, Micha and Sales26). Considering model 3 at the 100 % level, pre and post-modelled percentages of energy from more healthful grain foods in the present investigation were 1·5 % and 23·1 %, respectively (data not shown), which could represent a substantial predicted improvement in cardiometabolic health.
As found in previous dietary modelling studies, substitution models revealed potentially unwanted dietary effects(Reference Rehm and Drewnowski13,Reference Nordstrom and Thunstrom41) . In the present study intake of Fe, folate and vitamins B1, B2 and B6 would decrease if all the white rice and white bread consumed were substituted for brown rice and whole-wheat bread, respectively. In this sense, the results presented here support the balance between consumption of whole and refined grains in the diet in order to get the best nutritional composition possible from grain foods(Reference Jones, García and Braun42) However, even if 50 % of the population changed their white rice and white bread consumption, a decrease would be seen for vitamins B1 and B2, and it may be necessary to encourage the consumption of other sources of these nutrients, especially vitamin B1, which has a considerable prevalence of inadequacy among Brazilians (between 30 and 50 % of the population depending on age group)(Reference Araujo, Bezerra and Barbosa29,Reference Fisberg, Marchioni and Castro30) . Additionally, quality standards for whole-grain food production are required to ensure minimal losses during the milling process(Reference Ross, van der Kamp and King43). Possible losses of B vitamins may have contributed to the lower intake levels observed in post-modelled data. The majority of these nutrients is located in the bran and germ of the grain, which are removed during the refining process, and then recombined or reconstituted to produce whole-grain flours; incomplete recombination may result in lower-than-expected concentrations in whole-grain flours(Reference Seal, Nugent and Tee7,Reference Jones, Adams and Harriman44) .
The mandatory fortification of wheat flour with Fe and folic acid in Brazil may be one explanation for the lower intake of these micronutrients in the post-modelled estimations, since whole-wheat flour is not enriched due to technological issues(9,45) . Consistent with this, breads (including all types of refined breads) were among the main contributors to Fe and folate intake in the post-fortification period in Brazil(Reference Palchetti, Steluti and Verly46–Reference Vieira, Steluti and Verly48). Therefore, a combination of refined and whole grain foods may be the best way to mitigate the unwanted effects observed, or alternative methods for fortification of grains should be promoted for example during food processing(Reference Andersen, Koehler and Somoza49) or by biofortification(Reference Wakeel, Arif and Bashir50). From another perspective, the Brazilian diet comprises other sources of Fe and folate, such as beans, meat and vegetables, and dietary strategies aimed at improving the nutritional quality of grain foods consumed by the population must be aligned with actions to improve overall diet quality(Reference Souza, Pereira and Yokoo16,Reference Mozaffarian, Angell and Lang51) . In addition, dietary surveillance is essential to monitor dietary intake, evaluate interventions and shed light on future development of public health strategies.
Several approaches were used in previous modelling investigations focusing on grains or grain-based products. An improvement in diet quality was observed after substituting white bread, rolls, biscuits and spaghetti for equivalent whole wheat foods and after replacing white rice with brown rice in diets of adults living in the USA(Reference Thomson, Tussing Humphreys and Onufrak12). Solid foods consumed at breakfast were replaced with ready-to-eat cereals in data collected in the National Nutrition Examination Survey) and this resulted in higher intakes of whole grains (84·6 %), fibre (14·3 %), vitamin D (14·0 %), Fe (54·5 %) and folic acid (104·6 %) and led to a decline in intake of solid fats (–10·9 %). On the other hand, an unwanted increase in added sugars intake (5·0 %) was observed(Reference Rehm and Drewnowski13). By replacing refined grain ingredients with whole-grain ingredients in foods usually consumed by children in the USA, Keast et al. observed an increase of approximately 50 g/d of whole grains, and pre and post-modelled whole-grain intake were 6 % and 28 % of total grains intake, respectively(Reference Keast, Rosen and Arndt11). Recently, bread, pasta and ready-to-eat cereals were replaced with whole grain equivalent options in the United Kingdom National Diet and Nutrition Survey which significantly increased the intake of whole grains (from 23·9 g/d to 74·4 g/d) and fibre (from 18·3 g/d to 21·7 g/d)(Reference Mann, Yu and Hopkins14). Our findings corroborate with the previous literature, indicating that replacing refined grain foods with their whole-grain versions has the potential to improve diet quality. However, the impact on dietary intake at the population level will depend largely on intervention adherence.
Apart from the significant nutritional impact seen when modelling at 100 % change, partial substitution models, in which replacement was performed in 25, 50 and 75 % of the population, may provide a better representation of effects of such interventions on population dietary intake, given that individuals will respond differently to any dietary intervention(Reference Mozaffarian, Angell and Lang51). Substitutions made on a proportional basis indicate that important changes in nutrient intakes would be observed even if part of the population adheres to the proposed intervention. For example, increase in Mg intake would be observed if only 25 % of the population replaced their consumption of white bread and white rice with brown rice and whole-wheat bread, while mean dietary fibre intake increases from 50 % adherence level. Grain-based foods are the predominant food group in the Brazilian diet and account for approximately 40 % of total energy intake(Reference Fontanelli, Sales and Castro52). Together, white rice and white bread accounted for more than half (57 %) of the energy intake provided from grain foods(Reference Fontanelli, Micha and Sales26). Because of this central role in the Brazilian diet, it suggests that nutrition policy actions focused on these food items may provide wide-ranging effects on the population dietary intake. In particular, they may better target subgroups of the population with low intakes of more healthful grain foods, such as younger individuals, men, those with lower education and family income levels, and those reporting black, brown and indigenous ethnicity(Reference Fontanelli, Sales and Castro52). Development and evaluation of effective strategies to change such a deep-rooted eating habit deserves further investigation.
Multiple factors influence population food choices, and evidence suggests that policy measures emphasising personal responsibility are not sufficient to increase whole-grain intake, especially among countries, like Brazil, where-grain foods are traditionally consumed as refined grains(Reference Mozaffarian, Angell and Lang51,Reference Miller53) . Successful public health interventions aimed at increasing whole-grain intake comprised numerous stakeholder partnerships, specification of target intakes in dietary guidelines, labelling standards, food reformulation to increase the whole-grain ingredient content, educational materials, social media campaigns and events to familiarise communities with the taste of whole grain and preparation methods for whole-grain foods(Reference Suthers, Broom and Beck54,Reference Toups55) . In Brazil, initiatives to address the problem are beginning to emerge. For example, a formal definition of what constitutes a whole-grain food is under debate, and a new regulatory instrument for these products will be available soon in the country(56). This is a crucial step to help consumers chose healthy whole-grain options and support policy actions aimed at increasing population intake of more healthful grain foods.
Our analysis did not include information on the costs of brown rice and whole-wheat bread compared with the refined alternatives, but the proposed substitutions would probably increase dietary cost(Reference Harriman57,Reference Verly, Darmon and Sichieri58) . Considering that price strongly influence food choice, fiscal incentives for more healthful grain foods may be required in order to promote dietary change, especially among low-income subgroups(Reference Mozaffarian, Angell and Lang51). Another strategy to improve whole-grain intake is the inclusion of whole-grain foods in the basic food basket, and in already existing programmes, such as the National School Meal Program (Programa Nacional de Alimentação Escolar) and the Worker’s Food Program (Programa de Alimantação do Trabalhador). Increased whole-grain consumption may result in health improvement resulting in reduced health system burden and concomitant healthcare cost savings, for that reason, strategies to tackle the problem should be urgently implemented(Reference Lieffers, Ekwaru and Ohinmaa59,Reference Murphy and Schmier60) .
Strengths of the current study include the quality of the data used as input for the dietary modelling. This was derived from a representative sample of residents in a large metropolis of a middle-income country, where the low intake of whole grains was the leading dietary risk for death and disability-adjusted life-years in 2017(5). In addition, our previous study demonstrated that whole-grain intake is still far from recommended levels in this population(Reference Fontanelli, Sales and Castro52,Reference Mello, Sarti and Pereira61) , and this intake was associated with diet inequalities in São Paulo strongly suggesting that policy actions are required in this population(Reference Mello, Sarti and Pereira61). The strategies used to model an increase in the intake of more healthful grain foods took into account the particular composition of the Brazilian diet and considered the impact of varying levels of population adherence. Finally, the analysis covered a wide spectrum of the nutrient content of the diet.
Potential limitations should be acknowledged. First, dietary intake data were based on self-reported 24-h recalls, which include random and systematic errors, and are susceptible to misreporting of dietary intake(Reference Willett62). Refined grain foods may be more underreported, and as a result, post-modelled intakes could be underestimated(Reference Garden, Clark and Whybrow63). However, 24-h recalls were collected by trained interviewers using standardised methods to enable complete recalls, such as the Multiple Pass Method and standardised procedure to detail food items consumed(Reference Fisberg, Sales and Fontanelli18). Second, models were based on a single 24-h dietary recall. Therefore, we were not able to compare nutrient adequacy between observed and modelled nutrient intakes. In addition, the classification of participants according to their consumption of rice and bread, in particular brown rice and whole-wheat bread, does not distinguish between true nonconsumers and occasional nonconsumers of the study foods in question(Reference Willett62). Importantly, even with a single dietary recall, the study included a good representation of weekend day food consumption (˜31 %)(Reference Fisberg, Sales and Fontanelli18). Third, our analyses were based on standard versions of food items consumed by the Brazilian population and did not consider fortified foods, except for those fortified with Fe and folic acid, which fortification is mandatory. Fourth, the cost implication of the modelling outcomes was not considered in the modelling process and may have an impact on the translation of the models into real life.
Conclusions
Overall, the substitution of staple grain foods with more healthful options would lead to favourable changes in diet content of São Paulo residents. A significant increase in more healthful grain foods intake would be seen if the entire population consuming white rice and white bread changed their consumption to brown rice and whole wheat bread, respectively. However, substitution resulted in unwanted effects for B vitamins, and results support the balance between consumption of whole and refined grains in the diet. Our findings suggest that rice and bread are prime targets for policy actions aiming at increasing more healthful grain food intake in a Brazilian context.
Acknowledgements
Acknowledgements: We would like to thank all fieldworkers and all participants of the Health Survey of São Paulo. We also acknowledge the work on dietary data performed by the Evaluation of Food Consumption Research Group (Grupo de Avaliação do Consumo Alimentar) at University of São Paulo. Financial support: The 2015 Health Survey of São Paulo was supported by the São Paulo Municipal Health Department (grant number 2013-0.235.936-0), São Paulo Research Foundation (grant numbers 2012/22113-9, 2017/05125-7) and National Council for Scientific and Technological Development (grant numbers 472873/2012–1, 402674/2016–2, 301597/2017–0). This work was supported by São Paulo Research Foundation (grant number 2016/18742-1). Conflict of interest: There are no conflict of interest. Authorship: MMF, AMA, CHS and RMF conceptualized the study. MMF performed data management and statistical analysis. AMA, CHS and RMF supervised the analyses. MMF wrote the original draft. AMA, CHS, CJS and RMF critically reviewed the manuscript for important intellectual content. All authors approved the version to be published. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the School of Public Health, University of São Paulo, Brazil Institutional Review Board (certificate of presentation for ethical appreciation # 32344014.3.0000.5421, 36607614.5.0000.5421, and # 65484517.5.0000.5421). Written informed consent/assent was obtained from all participants.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980021001531








