


Anaemia affects pregnant women worldwide. The WHO recently estimated that 56·4 million pregnant women (41·8 %) globally were anaemic during 1993–2005(Reference de Benoist, McLean and Cogswell1). Anaemia during pregnancy is associated with adverse infant outcomes including low birth weight, preterm delivery and perinatal mortality(Reference Shobeiri, Begum and Nazari2–Reference Patra, Pasrija and Trivedi5), and it may also be associated with childhood intellectual disability(Reference Leonard, de Klerk and Bourke6). Severe anaemia is associated with maternal and child mortality(Reference Brabin, Prinsen-Geerligs and Verhoeff7).
China is the most populous country in the world. Research suggests that the prevalence of anaemia decreased from 1990 to 2000 among pregnant women in Asia and in China(Reference Mason, Rivers and Helwig8). However, in China, national data on the prevalence of anaemia among pregnant women are limited to only three studies(Reference Zhao, Yu and Liu9–Reference Li, Rao and Kong11), and the sampling methods in these studies were different, making comparison of the results difficult. Other Chinese studies on the prevalence of anaemia during pregnancy included women from only one city or province(Reference Yu12–Reference Pan, Wu and Xie14). In addition, information on the determinants of anaemia, other than time, is limited; most studies examine the trends in overall anaemia during pregnancy without regard to trimester(10, Reference McLean, Cogswell and Egli15).
The prevalence, causes and consequences of anaemia vary by trimester. A nationwide survey in China indicated that iron-deficiency anaemia is higher in the third trimester than earlier in pregnancy(Reference Xiong, Buekens and Fraser16). Anaemia in the first and second trimesters, but not in the third, is associated with low birth weight, preterm delivery and stillbirths(Reference Xiong, Buekens and Fraser16–Reference Tomashek, Ananth and Cogswell18).
The purpose of the present study is to report the prevalence and determinants of anaemia among Chinese pregnant women in two provinces from 1993 to 2005. Information on the prevalence and determinants of anaemia will help to inform appropriate interventions to prevent pregnancy-related anaemia in China.
Methods
Data sources
The perinatal health-care (PHC) surveillance system was established in twenty-seven counties or cities in Hebei, Shanxi, Jiangsu and Zhejiang provinces in 1992 as part of the China–US Collaborative Project funded by the US Centers for Disease Control and Prevention (CDC)(Reference Berry, Li and Erickson19, Reference Zheng, Wang and Ji20). All women were enrolled in the PHC system in the county hospital or county maternal and children health-care institute when they first sought care for their pregnancy or before getting pregnant. All women in the system were given a unique PHC identification number (PHC ID). Our study subjects were women who resided in fourteen cities or counties in Jiangsu and Zhejiang provinces, participated in the PHC surveillance system and delivered babies from 1 January 1993 to 31 December 2005. This surveillance system captured information on demographic characteristics, medical history and pre- and postnatal visits. Hb concentration was measured at premarital, prenatal and postnatal visits. The present study focuses on Hb concentration during the prenatal visits.
Exclusions
Over the 13-year period, 891 640 women were registered in the surveillance system and delivered babies. Those who enrolled in the PHC system after delivery (30 567 cases), had a missing delivery date (3546 cases) or had no Hb recorded at any time during pregnancy (2722 cases) were excluded from the present study. Another 390 470 women were excluded because they were missing a recorded Hb value in one of the three trimesters. After exclusions, a total of 467 057 women (52 % of the original group) remained in the analysis. Compared with women who were excluded, the absolute difference in prevalence in the first, second and third trimesters was 3·9 %, 1·6 % and 0·1 %, respectively.
Hb concentration and anaemia diagnostic criteria
Capillary blood Hb concentrations were measured when women visited the township or county hospitals during or after pregnancy. Each woman included in the present analysis had one Hb test in the first trimester and at least one Hb test in each of the second and third trimesters. Before 2000, only the lowest Hb concentration was recorded in the woman’s health-care booklet for the PHC surveillance system if she had more than one Hb concentration measured in the second or third trimester. The PHC system became electronic in 2000, and all of the Hb concentrations were captured. To maintain consistency over time we used the lowest Hb concentration. In accordance with the WHO(21) and the International Nutritional Anemia Consultative Group Steering Committee criteria(22), anaemia in the first and third trimesters was defined as an Hb concentration <110 g/l, and anaemia in the second trimester was defined as an Hb concentration <105 g/l. In all trimesters, moderate anaemia in pregnant women was defined as an Hb concentration <90 g/l; severe anaemia, <70 g/l; and very severe anaemia, <40 g/l.
Definitions
The prevalence of anaemia was defined as the proportion of women whose Hb was below the criteria for each trimester divided by the total number of women who were tested for Hb in the same trimester. We randomly selected one Hb record of the three trimesters to calculate the overall prevalence of anaemia and the anaemia was determined according to the criteria of the trimester when it was measured. To examine trends in anaemia prevalence, we used date of delivery to compare the anaemia prevalence by trimester and year within the same sample of women.
Statistical analysis
All statistical analyses were performed using the SPSS for Windows statistical software package version 11·5 (SPSS Inc., Chicago, IL, USA). We used the χ 2 test to examine differences in anaemia prevalence by sociodemographic characteristics (e.g. place of residence and occupation) and calculated unadjusted relative risks (RR) to determine the magnitude of these associations. We used the trend χ 2 test to determine whether secular trends in anaemia prevalence were statistically significant. Multiple logistic regression models were used to examine secular trends from 1993 to 2005, adjusting for potential confounders: occupation, education, age, gravidity, province and location (urban, suburban or rural). Because of its correlation with gravidity and the large proportion of missing values (31·1 %), parity was not included in this model.
Results
The mean age of women at the time of delivery was 25·2 (sd 3·4) years. The mean gestation at delivery was 39·3 (sd 1·6) weeks. The proportion of women who were farmers declined from 86·0 % in 1993 to 65·7 % in 2005, and the proportion of women who had higher education (including college and high school) and who lived in urban areas increased (Table 1, P < 0·001 for differences in proportions for all three characteristics before and after 2000).
Table 1 Demographic characteristics of pregnant women in south-east China, stages 1993–1999 and 2000–2005Footnote *
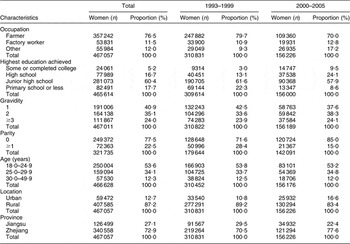
* Women whose variable value was missing were not included in the calculation of proportion.
Anaemia prevalence by trimester
The overall anaemia prevalence was 39·6 % (95 % CI 39·5, 39·7) from 1993 to 2005. Anaemia prevalence increased from the first trimester (29·6 %, 95 % CI 29·5, 29·8) to the second (33·0 %, 95 % CI 32·9, 33·2) and third trimesters (56·2 %, 95 % CI 56·1, 56·4, trend χ 2 test P < 0·001). The prevalence of moderate and severe anaemia was 0·1 % in the first trimester, 0·2 % in the second trimester and 0·3 % in the third trimester during 1993–2005.
Secular trends in anaemia prevalence
Anaemia prevalence declined from 1993 to 2005 (Table 2). The overall prevalence of anaemia declined from 54·5 % in 1993 to 26·6 % in 2005, a 51·2 % decrease. The anaemia prevalence declined most in the first trimester, from 53·3 % in 1993 to 11·4 % in 2005, a 41·9 percentage point change and a relative decrease of 78·6 %. The decline occurred in the prevalence of mild anaemia, and the prevalence of moderate–severe anaemia was consistent over time.
Table 2 Secular trends in anaemia prevalence (%) by pregnancy trimester among women in fourteen cities in Jiangsu and Zhejiang provinces, China, 1993–2005

*% anaemic in 2005 minus % anaemic in 1993.
†(Absolute change divided by the % anaemic in 1993) × 100.
The prevalence of mild anaemia decreased significantly, and the prevalence of moderate–severe anaemia varied between 0·1% and 0·2% in the first, 0·1% and 0·3% in the second and 0·2% and 0·4% in the third trimester during 1993–2005.
Secular decreases in anaemia prevalence were seen across all trimesters, regardless of the sociodemographic subgroup (Table 3). The prevalence of anaemia varied little by sociodemographic characteristics, and the relative differences were small, less than a 1·25 relative increase in the prevalence of anaemia.
Table 3 Absolute and relative declines in anaemia prevalence (%) among pregnant women by sociodemographic characteristics and trimester, fourteen cities in Jiangsu and Zhejiang provinces, China, 1993–2005

*% Anaemic in 1993 minus % anaemic in 2005.
†(Absolute change divided by the % anaemic in 1993) × 100.
The prevalence of anaemia was lower among women with college education than among women with less education (for overall prevalence, RR = 0·74, 95 % CI 0·72, 0·75) and among women who lived in urban v. other areas (for overall prevalence, RR = 0·74, 95 % CI 0·73, 0·75). The overall anaemia prevalence among women 25·0–29·9 years of age was lower than among women who were 30·0–49·9 years of age (RR = 0·73, 95 % CI 0·71, 0·74). Other differences in secular decreases by sociodemographic characteristics did not appear to be consistent across trimesters.
Logistic regression analyses indicated that year was associated with anaemia prevalence. The odds of anaemia declined on average by 15 %, 7 % and 5 % per year in the first, second and third trimesters, respectively, before and after adjusting for the sociodemographic characteristics (Table 4).
Table 4 Crude and adjusted OR for anaemia prevalence per year by trimester (n 453 812 women)
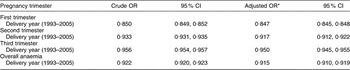
*Separate multiple logistic regression models for each trimester and overall were used to estimate the OR for anaemia by year adjusted for the following sociodemographic characteristics: occupation, education, age, gravidity, province and region.
Discussion
We found that the prevalence of anaemia among pregnant women in south-east China decreased from 1993 to 2005 in all trimesters among women in all age, education, occupation and geographic groups. Despite these declines, however, the prevalence of anaemia in 2005 was still at a level of public health concern in all trimesters.
The overall anaemia prevalence in our study was similar to that of some studies in China before 2000(10, Reference Yu12, 23) and in a 2006 report(Reference Zhao, Yu and Liu9), but it was higher than that in the 2002 Chinese Nutrition and Health Survey in similar areas(Reference Yin, Lai and Ma24). The regions in the present study belonged to the first class economic conditional rural area in the Chinese Nutrition and Health Survey. In that survey, the prevalence of anaemia among pregnant women was found to be 22·7 %, 37·1 % lower than the prevalence among women in our study in the same year (36·1 %). There are two possible explanations for this discrepancy. First, we selected the lowest Hb concentration per woman from the measurements recorded in each of the second and third trimesters, which may have biased our results downwards. Second, data from the 2002 Chinese Nutrition and Health Survey include women in a broader geographic area.
The reasons for the decline that the present study found in anaemia prevalence during pregnancy are not understood, but they may include changes in sociodemographic characteristics associated with changes in diet, and general improvement in diet across the entire population. We did not collect information on diet, but another study(Reference Liu, Wang and Wang25) on dietary changes of Chinese residents suggests a decrease in the percentage of dietary energy supplied by cereals and an increase in the percentage supplied by fat intake per capita, especially from animal foods, a good source of dietary iron. In addition, studies in China indicate that maternal education is associated with nutritional knowledge, attitude and practice(Reference Liu, Wang and Wang25, Reference Yin, Li and Jin26), and that urban residence is associated with increased consumption of foods high in protein(Reference He, Zhai and Wang27). Both the level of education and the proportion of women living in urban areas increased in our study.
Secular trends in first-trimester anaemia prevalence are consistent with the changes in anaemia prevalence at the premarital health examination(Reference Xu, Jin and Ye28). Anaemia prevalence in the first trimester declined to less than that in the second trimester in 1996. This suggests that changes during the study period were more likely to affect anaemia in early pregnancy than during the second and third trimesters. In normal pregnancy, the expansion of the plasma volume that precedes the increase in red cell mass creates a disproportionate expansion of plasma volume (50 %) compared with the increase in red cell mass (30 %). Therefore, Hb values start to decline during the early part of the first trimester and reach their nadir near the end of the second trimester and early part of the third trimester. In the last trimester of pregnancy, the rate of increase in plasma volume reaches a plateau, but the red cell mass continues to rise, resulting in a constant increase in the Hb level, which may reach normal levels at term. But the prevalence of anaemia observed in the present study was not decreased (the mean values of Hb in the third trimester were not higher than the mean Hb in the second trimester) in the third trimester. This may be associated with the deficiency of related nutrients such as iron, folic acid and vitamin A. In addition to the overall changes in diet, another change that may be associated with declines in the prevalence of first-trimester anaemia is the implementation of the China–US Collaborative Project for Neural Tube Defect Prevention from 1993 to 1996(Reference Berry, Li and Erickson19). For 2 years, women in twenty-one counties or cities in Jiangsu, Zhejiang and Hebei provinces (the fourteen counties or cities of our study were among them) who participated in the programme consumed 400 μg of folic acid daily during the periconceptional period. We would have liked to investigate whether folic acid contributed to the decline in anaemia prevalence, but we had no information on women’s use of folic acid during the other 11 years of the present study. We know of no other special anaemia-prevention programmes (e.g. fortification of foods) that occurred in the study area during the 13-year study period. Iron tablets were not routinely prescribed for women during pregnancy unless they were anaemic. Although we did not collect data on prenatal supplement use, the proportions of pregnant women who consumed prenatal folate and iron supplements were about 30 % and 14 %, respectively, in the first class economic conditional areas in the 2002 Chinese Health and Nutrition Survey(Reference Yin, Lai and Ma24).
Data from studies among women who received adequate iron supplementation during pregnancy indicate that Hb decreased in the second trimester, but increased again in the third trimester(Reference Sharma, Jain and Mallika29–Reference Madhavan, Bhaskaram and Balakrishna31), and that iron supplementation increased average Hb concentration among pregnant women(Reference Mason, Rivers and Helwig8, Reference Graham, Haskell and Pandey30, Reference Bhutta, Ahmed and Black32). In our study, Hb concentration declined from the first trimester to the third trimester. Along with the slower decline over time for second- and third-trimester anaemia relative to first-trimester anaemia, our results suggest that it may be necessary to strengthen nutrition interventions before and during pregnancy to prevent anaemia among women in these two areas of China.
The present study has several strengths. First, most of the women in our study were enrolled in the PHC surveillance system before pregnancy; thus, we had data on anaemia during all trimesters for a large proportion of the women in our study. Second, these data provide information on trends in anaemia prevalence among a large population of women over more than 10 years. Third, the measurement of Hb concentration was consistent with accepted methods(23). In 1991, the China Ministry of Health required that the haemiglobincyanide test be used in all laboratories in county hospitals(33); routine quality control was implemented at the same time. Since 1998, automatic blood analysers have been widely used in hospital laboratories in south-east China.
Our study is subject to several potential limitations. First, because we studied only women who had an Hb concentration in all three trimesters, almost half the women were excluded from the analysis. Although the prevalence of anaemia was somewhat lower among excluded women than among those who were included, the trends over time did not differ between the two groups. By including only women with Hb measurements in all three trimesters, we were able to compare differences in secular anaemia trends across all three trimesters among the same women. Second, the number of women with Hb measurements appeared to decline over time. This decline appears to correspond with the decrease in the number of births within these two provinces(Reference Xia34, Reference Wu35), rather than the differences in the proportion of women who were included in the PHC surveillance system. To account for changes in the population over time, we stratified our analysis by demographic characteristics. Third, although iron-deficiency anaemia has been shown in other studies to be the most common cause of anaemia in pregnant women in China(Reference Pan, Wu and Xie14, Reference Liao36), other nutrient deficiencies(Reference McLean, Cogswell and Egli15, Reference van Gellekom, Lindauer-van der Werf and Hague37) (e.g. folate, vitamin B12 and vitamin A), infections and environmental factors (e.g. exposure to heavy metals) may associate with anaemia in pregnant women. As we did not collect data on these potential causes in the present study, the exact causes of anaemia are unknown in this population. Fourth, some women contributed data from more than one pregnancy, but the proportion of these women is very likely low given the high percentage of women who were nulliparous. We found similar trends over time in the prevalence of anaemia by parity. In 1993, the prevalence of anaemia decreased from the first to the second trimester and then increased in the third trimester. However, starting in 1995, the prevalence of anaemia in the second trimester is the same or higher than the prevalence in the first trimester. This finding could potentially be due to the fact that the PHC surveillance system was just newly established in 1992 and the health-care booklets were revised in October 1993 because some variables were not collected correctly. This could potentially lead to some discrepancies in the Hb numbers, thereby affecting our estimates.
Finally, although the sample of pregnant women was quite large, our study covered only two provinces in south-east China and because south-east China is one of the wealthier regions of the country based on the economic development(Reference Xu and Jia38, 39), our results are not generalizable to all pregnant women in China.
According to the WHO(23), anaemia is a moderate public health problem if its prevalence in a population is 20·0–39·9 %, and it is a severe problem if the prevalence is higher than 40·0 %. From 1993 to 2005, anaemia prevalence improved from severe to moderate status in pregnant women in two provinces in south-east China. The national survey on nutrition of children and women in 2006(Reference Zhao, Yu and Liu9) indicated that anaemia prevalence in pregnant women was the lowest in eastern areas of China and was more than 40·0 % in the middle and western areas. Therefore, the prevalence of anaemia in the entire population of pregnant women in China is likely to be significantly higher than what we found in the present study.
Conclusion
The prevalence of anaemia among pregnant women in Jiangsu and Zhejiang provinces decreased substantially from 1993 to 2005, especially during the first trimester of pregnancy. However, anaemia in the third trimester is still a severe public health problem among pregnant women in these areas, especially among women who are farmers and who have less education. Despite significant progress in reducing the prevalence of anaemia, additional nutritional and other interventions, e.g. improving the educational status of women, should focus on interventions before pregnancy and early in pregnancy to boost iron stores in China.
Acknowledgements
The present study was funded by the CDC Grant U11/CCU015586-02. The authors declare no conflict of interest. L.J. conceived the idea of the manuscript and led the analysis, interpretation and writing of the manuscript. M.E.C., L.F.Y., R.Y. and J.L. contributed to the analysis, interpretation and writing of the manuscript. Other co-authors contributed to the review of the manuscript. The authors thank all the persons working in the Maternal and Child Health stations in the fourteen counties or cities during 1993 through 2005, including Taicang, Wujiang, Kunshan and XiShan in Jiangsu province, and Jianxing, Xiuzhou, Pinghu, Tongxiang, Haining, Cixi, Ninbo, Yinzhou, Jiashan and Haiyan in Zhejiang province, who collected all the data used in the present study.




