



Introduction
The goal of home-based hospice care is to provide end-of-life palliative care, improving quality of life (QoL) for patients with serious illness and a life expectancy of 6 months or less (Zeng et al. Reference Zeng, Wang and Ward2018). Palliative care focuses on providing symptom relief, while addressing the distress of both patients and their caregivers. These include emotional suffering and existential distress, with a loss of meaning, autonomy and dignity; hopelessness; and death-related anxiety, all of which can result in impaired QoL, demoralization, and in some cases even suicide (Grassi et al. Reference Grassi, Sabato and Caruso2022). The home hospice cancer care setting presents many challenges to patients, their informal caregivers (e.g., family members), palliative health-care providers (HCPs), and the patient’s family physician. For some patients and their informal caregivers, entering hospice care setting can signify a dramatic change, where end-of-life care moves toward an emphasis on improving QoL rather than outcomes such as survival or “cure” (Yang et al. Reference Yang, Zhao and Cui2021). A qualitative study of a hospice care setting described the patient experience of a transformative process, from initial reluctance into acceptance and “restoration of an identity that expands beyond the ‘sick’ role” (Vasileiou et al. Reference Vasileiou, Smith and Kagee2020). The study presented stereotypic perceptions of the hospice setting as one associated with death and dying; and the interactions between patients and medical staff addressing only QoL-related concerns. In another qualitative study conducted in 3 home-based palliative care programs in Ethiopia, both patients and caregivers reported limited psychosocial, emotional, spiritual support, while emphasizing physical complaints such as pain and gastrointestinal concerns (Kaba et al. Reference Kaba, de Fouw and Deribe2021).
Informal caregivers of patients in hospice care may also undergo a transformative process, experiencing the challenges associated with the need to engage with professional caregivers, while navigating the home-based system in order to access resources and supporting services (Mohammed et al. Reference Mohammed, Swami and Pope2018; Wennman-Larsen and Tishelman Reference Wennman-Larsen and Tishelman2002). A qualitative study examining older patients with cancer and their family caregivers identified subthemes in caregiver narratives such as “Knowing and Doing,” and “Caring for the Caregivers.” These were associated with a positive impact on physical, emotional, and social well-being (Jack et al. Reference Jack, Mitchell and Cope2016). Isenberg et al identified “enablers and disablers,” within the caregiver role; uncertainty; and financial resources, which could significantly increase or decrease the likelihood that the needs of the patient were being met (Isenberg et al. Reference Isenberg, Killackey and Saunders2021). In a meta-ethnographic qualitative study of a hospice care setting, it was concluded that the presence and competence of the palliative care HCP were the main components leading to a sense of security which was shared by both patients and their caregivers (Sarmento et al. Reference Sarmento, Gysels and Higginson2017). Specific end-of-life concerns, such as issues related to diet, were systematically identified in a mixed-methods study which identified unmet needs in the provision of nutritional care (Hui-Lin and Ting Reference Hui-Lin and Ting2022). These, in addition to difficulties in HCP-related communication, were considered a leading theme in a US qualitative study exploring the experiences of bereaved parents of pediatric oncology patients at the end of their child’s life (Sedig et al. Reference Sedig, Spruit and Paul2020).
Research on the perspectives of palliative care HCPs regarding expectations among patients and caregivers in hospice care is limited. In a qualitative study among HCPs in Germany, Steven et al. identified a number of HCP communication-related challenges in an advanced palliative care setting, recognizing the need for further coaching and support programs to improve the quality of communication in palliative care (Steven et al. Reference Steven, Lange and Schulz2019). Reblin et al. explored the 3-way communication between patients, spouse-caregivers, and nurses during home hospice visits, identifying varying degrees of expressing distress (Reblin et al. Reference Reblin, Clayton and Xu2017). Informal caregivers have been shown to score the patients’ QoL-related concerns more severely (Ishida et al. Reference Ishida, Sato and Komatsu2022), though caregiver burden and positivity may affect their assessment, especially regarding psychological patient domains (Higginson and Gao Reference Higginson and Gao2008). In a study examining a geriatric palliative oncology setting, only partial concordance was found for symptom assessment by patients and their nurses and physicians (Pautex et al. Reference Pautex, Berger and Chatelain2003).
Hudson et al. suggested that the hospice nurse may play a significant role in mediating patient–caregiver communication-related conflicts, while navigating emotional-related concerns (Hudson et al. Reference Hudson, Reblin and Clayton2019). Wyatt et al. described how general medical practitioners described managing patients’ and caregivers’ expectations in end-of-life care as a significant challenge, particularly when the role of the primary care physician in palliative care was not clear (Wyatt et al. Reference Wyatt, Bastaki and Davies2022).
Oncology and palliative care services in Israel are provided without cost to patients, as part of the national health-care coverage. Palliative care is a recognized subspecialty for both physicians and nurses, with palliative services offered to patients in both community (palliative care clinics and home hospice services) and hospital settings. Cross-cultural aspects of palliative care are particularly challenging in northern Israel, where about half of the population is Jewish (some Israeli born, with a large community of Russian-speaking patients) and half Arab (Muslim, Christian, or Druze), with widely differing demographics, religiosity, and health-belief models of care (Hajjar et al. Reference Hajjar, Charalambous and Baider2015).
The present study adopted a combined qualitative and quantitative methodological approach to identify patient concerns and unmet needs in the home hospice care setting, while exploring perspectives of informal caregivers and HCPs. The implications regarding implementation of the study findings in medical training of palliative HCPs are discussed, and communication barriers addressed.
Methods
Study design and setting
The study was conducted using a pragmatic (noncontrolled, non-randomized) research methodology. Participants were recruited from September 2016 to May 2017 at the Home Care Hospice, Clalit Health Services, Haifa and Western Galilee District, Clalit Healthcare Services, Israel. Patients aged ≥18 years diagnosed with cancer and admitted within the previous 2 months to the home hospice care program were deemed eligible for study inclusion. Informal caregivers, palliative HCPs working in the study home hospice care setting and the patient’s family physicians were eligible for study inclusion as well.
Primary study outcome
The primary study objective was the identification of concerns and symptoms which patients felt were not adequately addressed in the home hospice care setting. The study hypothesis (H0) was that in this specific culturally diverse group, the patient’s informal caregiver, the palliative HCP, and the family physician would assess the patient’s distress differently from the patient, as well as from each other.
Assessment of patient QoL-related symptoms and concerns
Patient QoL-related symptoms and concerns were assessed among participating patients, informal caregivers, palliative care HCPs (physician or nurse), and the patient’s family physician. Quantitative assessment of these concerns was conducted using the Edmonton Symptom Assessment Scale (ESAS) (Bruera et al. Reference Bruera, Kuehn and Miller1991; Oldenmenger et al. Reference Oldenmenger, de Raaf and de Klerk2013) and the Measure Yourself Concerns and Wellbeing (MYCAW) questionnaire (Paterson et al. Reference Paterson, Thomas and Manasse2007). The ESAS and MYCAW questionnaires were translated bidirectionally from the original English version to Hebrew by 2 independent physicians, both fluent (at a mother tongue level) in English and Hebrew (Ben-Arye et al. Reference Ben-Arye, Schiff and Silbermann2015). The same translation bidirectional translation was conducted from English to Russian (Sharabi et al. Reference Sharabi, Levin and Schiff2016), and to Arabic (Ben-Arye et al. Reference Ben-Arye, Massalha and Bar-Sela2014).
The principal study investigator (JD) is the director of the Home Care Hospice, and is fluent in Arabic, Hebrew, and Russian. JD conducts an initial palliative care intake at the patient’s home, assessing QOL-related concerns, as well as those assessed by their informal caregivers, using the ESAS and MYCAW questionnaires. Patients and informal caregivers are instructed to complete these assessments independently, while encouraging them to ask JD for clarifications when needed. Using the QoL assessments, JD then designs a palliative care treatment plan, assigning a team of physicians, nurses, and social workers, based on their availability. The ESAS tool asks patients to score the severity of 10 symptoms, from 0 (lowest severity) to 10 (greatest severity). The MYCAW tool asks patients to list their 2 most important concerns, scoring them from 0 (doesn’t bother me at all) to 6 (bothers me greatly).
Qualitative assessment was conducted using short narratives of participants from each of the 4 groups of study participants. This entailed 2 open-ended questions which are part of the follow-up MYCAW questionnaires, asking respondents to describe “other things affecting your health“; and “what has been the most important aspect (of the therapeutic process) for you?.” Study participants were also asked about the main concerns facing the patient over the past 2 weeks; and to what extent these concerns and needs were (or were not) being addressed by the medical team? All 4 groups of participants were asked to describe how they see both the “full” as well as the “empty half of the glass,” exploring gaps in communication and redefining treatment goals.
Data analysis
The sample size of the study was calculated using the OpenEpi program (Microsoft). It was determined that in order to measure differences between patients and HCPs with the ESAS-general well-being score, at least 22 participants would be needed in each arm of the study. This would allow an alpha-error of 0.05 and beta-error of 0.2 (power 80%) to detect a difference of 1.5 points on a 0–10 point ESAS scale, assuming a scale of 7 ± 2 in one group, compared with 5.5 ± 1.5 in the other. Quantitative assessment comparing the 4 study groups vis-à-vis the patient’s concerns was based on ESAS and MYCAW scores. Assessment was performed at study entry with no follow-up, precluding intragroup analysis. An intergroup analysis was thus performed with Kruskal–Wallis test referring to multiple comparisons, considering each ESAS scale separately while comparing the 2 groups. This, in contrast with analysis of variance for multiple dependent variables and multivariate analysis of variance (MANOVA) procedure. No matching between patients, caregivers, HCPs, and family physicians was performed, considering the small sample size (e.g., of the family physician group). A t-test was used to determine differences in continuous variables when normality was assumed; a Mann–Whitney U test for abnormal distribution. P values of <0.05 were considered statistically significant.
Qualitative assessment was based on the short narratives provided in the second section of follow-up MYCAW questionnaires (Keshet et al. Reference Keshet, Schiff and Samuels2015). A conventional content analysis was employed, with coding categories derived inductively directly from the text data (Hsieh and Shannon Reference Hsieh and Shannon2005). The advantage of this approach is that it enables deriving information directly from study participant responses, without imposing theoretical perspectives or preconceived categories. It also enabled flexibility in category development, giving voice to the respondents. The content analysis was conducted by YK, a medical sociologist with an expertise in qualitative research in supportive cancer care and integrative oncology, using the ATLAS.ti version 8 textual data analysis software (ATLAS.ti Scientific Software Development, Berlin, Germany).
Ethical considerations
The study protocol was approved by the Ethics Review Board (Helsinki Committee) at the Clalit Health Services, Israel (research registration COM-14-0058). Participation was open to all patients, caregivers, and medical professionals, regardless of age, gender, sexual preference ethnicity, or religious persuasion.
Results
Description of the study group
A total of 24 patients undergoing home hospice care were recruited, along with 22 informal caregivers; 22 palliative HCPs (17 physicians, 5 nurses); and 11 family physicians, for a total of 78 participants. Rates of participation among informal caregivers was 91.6%; palliative HCPs 91.6%; and family physicians 45.8%. It should be noted that all patients were registered with a family physician, regardless of their home hospice care.
The mean age of the patient cohort was 75.2 ± 10.7 years, with equal gender distribution. Most patients self-identified as Jewish (83.3%); religiously secular (58.3%); born outside of Israel (56.5%); and with Hebrew as their primary language (13.54%). Most patients did not have an academic education (62.5%), and were of a low-income status (52.5%). The primary site of cancer varied among this cohort, with most diagnosed with cancer of the gastrointestinal tract (45.8%). The majority of patients (62.5%) reported having undergone treatment with complementary and alternative medicine during their hospice care, with less than half (47.8%) reporting having had experience with these modalities in the past.
Quantitative assessment of QOL-related concerns
Table 1 presents a comparison of scores for QoL-related concerns among patients, as scored by the 4 study groups completing ESAS and MYCAW questionnaires, as well as a comparison between patients and their informal caregivers. Informal caregivers reported higher ESAS fatigue scores when compared with patients (8.5±1.6 vs. 7±2.4, p =0.009). A similar trend with borderline statistical significance was also observed with higher (i.e., more severe) symptom scores among informal caregivers for ESAS anxiety (p =0.063), sleep (p =0.059), and general well-being (p =0.061). At the same time, family physicians gave lower ESAS scores for drowsiness than patients (p =0.046) and palliative HCPs (p =0.009). Family physicians also gave lower ESAS sleep scores when compared with informal caregivers (p =0.035); and MYCAW well-being scores when compared to patients (p =0.021).
Table 1. Comparison of scores for symptom severity among the 4 study groups regarding patient QoL-related concerns (see text)
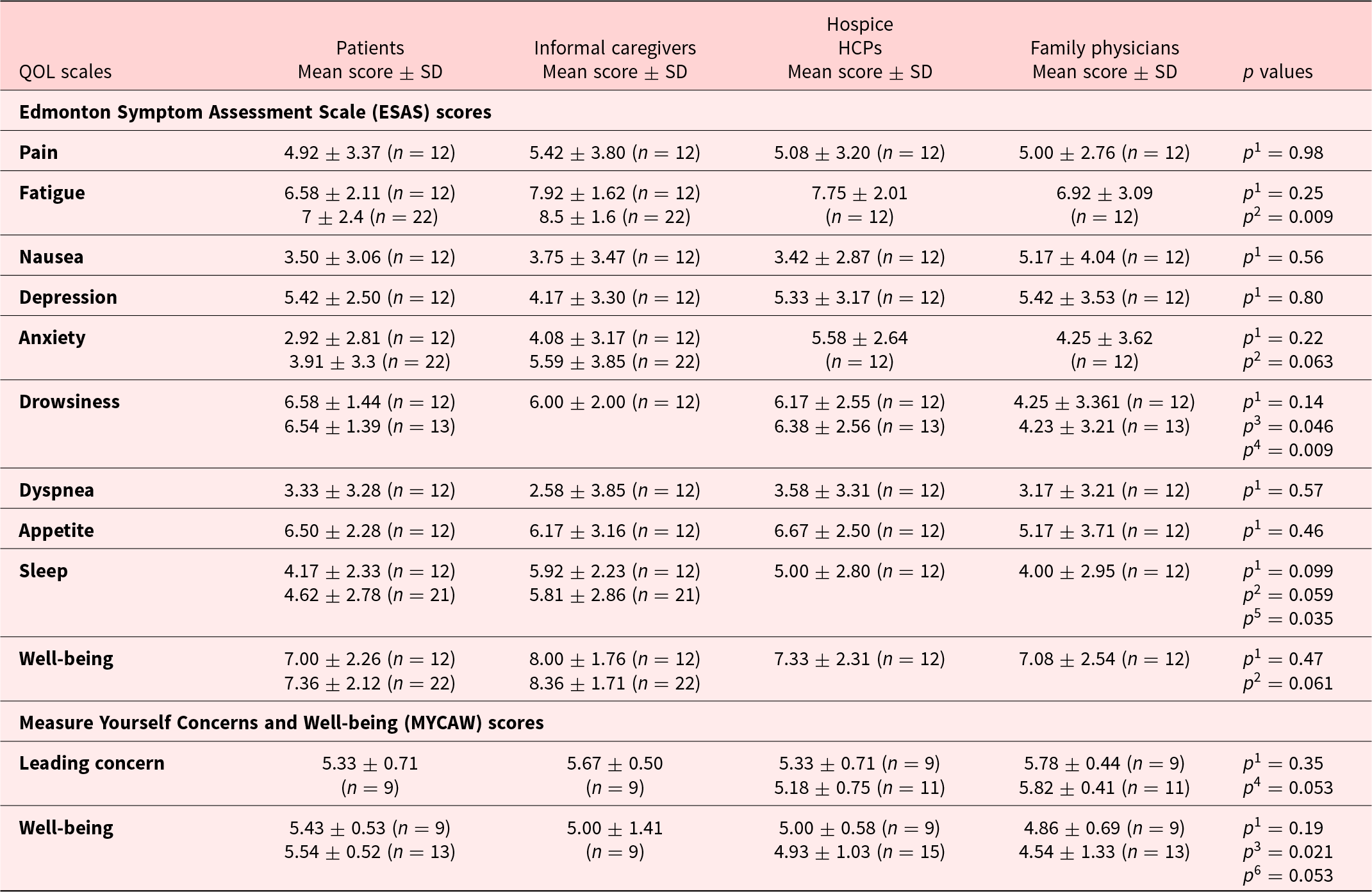
HCP = health-care provider; analysis was performed comparing variables reported by all quartet members on ESAS (12) and MYCAW (9); additional data is presented relating to dyads of patients and informal caregivers.
p 1 = comparison of the 4 groups.
p 2 = compared patients and caregivers groups.
p 3 = compared patients and family physicians groups.
p 4 = compared family physicians and hospice HCPs.
p 5 = compared caregivers and family physicians.
p 6 = compared patients and hospice HCPs groups.
Table 2 presents the leading QoL-related concerns (by percent) reported by patients on MYCAW questionnaire. These included emotional-spiritual (41.7% of patients); gastrointestinal (including appetite loss, 41.7%); and fatigue-related symptoms (37.5%). Patients were less likely than palliative HCPs to report emotional and spiritual concerns (77.2% vs. 41.7%, p =0.02); and more likely to report functional (p =0.049) and gastrointestinal (p =0.05) concerns. This discrepancy is also presented in Figure 1 with respect to the percentage of total MYCAW-reported concerns as listed in each of the 4 study groups. Patients were more likely than palliative HCPs to list on gastrointestinal/appetite (p =0.05) and daily function-related concerns (p =0.048). Patients tended less to include emotional-spiritual concerns in their MYCAW questionnaires when compared to palliative HCPs (p =0.15) and family physicians (p =0.29), though this observation did not reach statistical significance.
Table 2. Comparison of perspectives among the 4 groups regarding leading patient concerns on MYCAW (see text)
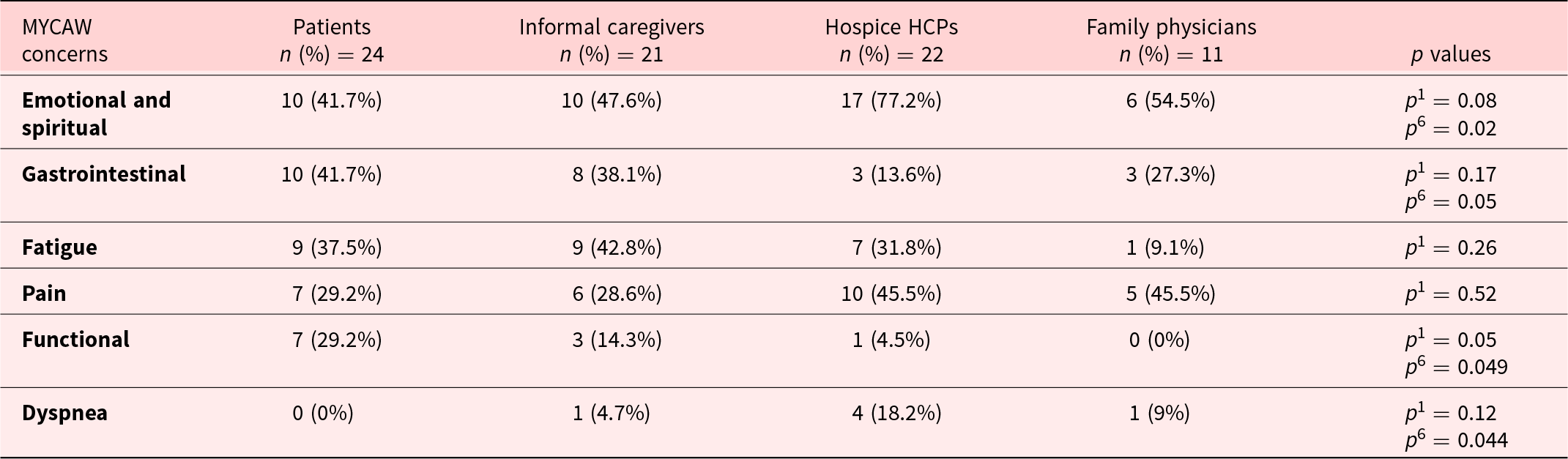
MYCAW concerns present the percentage of interviewees in each quartet section reporting specific concern (% of patients rather than % of total concerns).
HCP = health-care provider; MYCAW = Measure Yourself Concerns and Well-being.
p 1 = comparison of the 4 groups.
p 2 = compared patients and caregivers groups.
p 3 = compared patients and family physicians groups.
p 4 = compared family physicians and hospice HCPs.
p 5 = compared caregivers and family physicians.
p 6 = compared patients and hospice HCPs groups.

Figure 1. MYCAW concerns.
Qualitative assessment of QOL-related concerns
Study respondents mentioned different types of hardships, with a number of factors emerging from the analysis which were reported to be helpful in dealing with these hardships. These include the patient’s ability for self-help, as well as help provided by family members and friends, and by the medical care team, primarily family doctors and the hospice staff. At the same time, a number of factors which were not felt to adequately address the needs of patient in the hospice-care setting were also identified by the study respondents. These included helping them deal with the fear of death; difficulties related to the family dynamic; and dissatisfaction with the treatment provided by doctors and hospice staff (Figure 2).
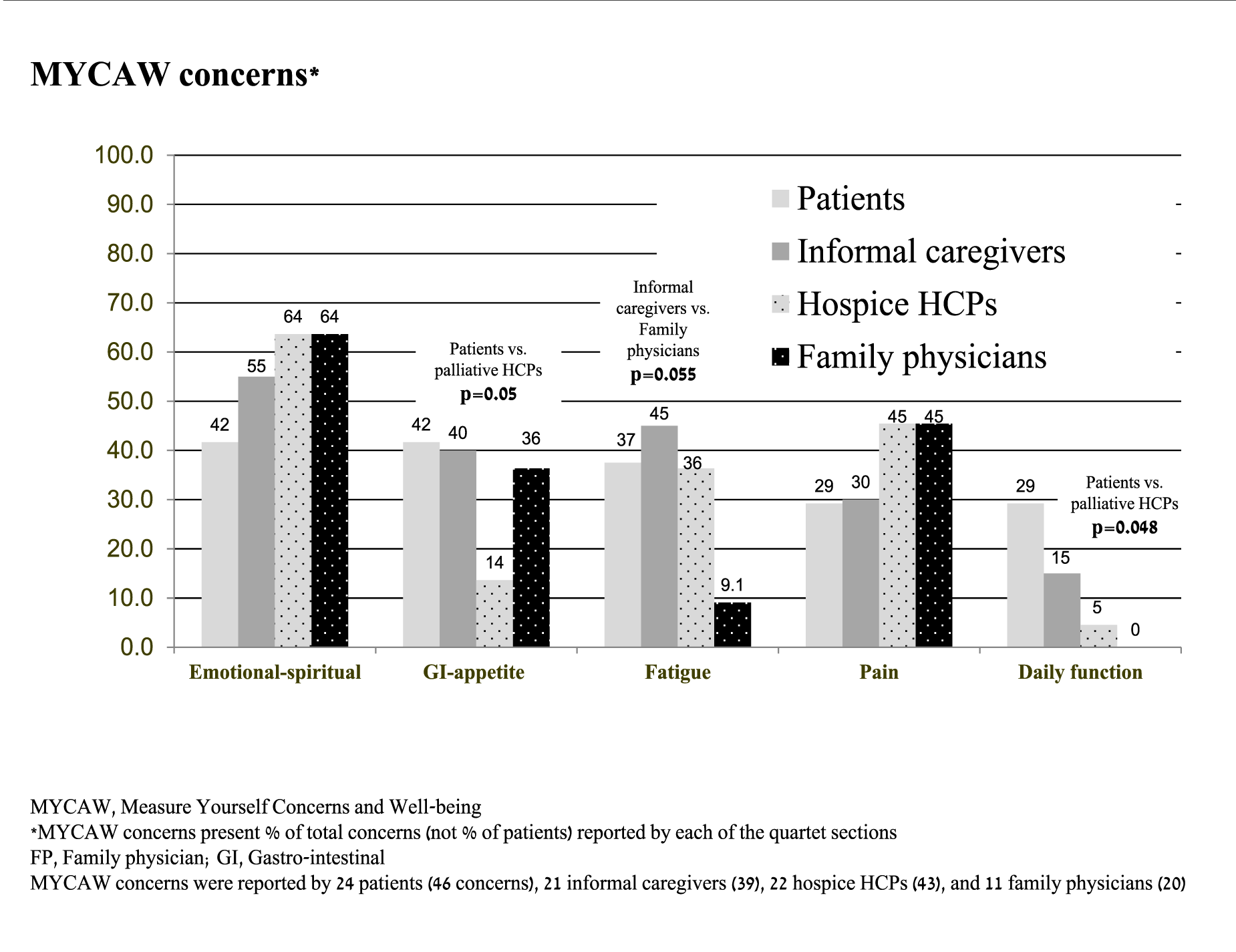
Figure 2. Qualitative assessment code book.
Most of the short narratives derived from the second part of the follow-up MYCAW questionnaires emphasized the importance of available resources, both internal as well as external, which patients could access to better cope with QoL-related concerns.
Patients and informal caregiver narratives described how self-care and a will to live help them cope with their malignancy. One patient described this as “the spirit of anchoring.”
What gives me strength is the spirit of anchoring. I go to the mirror and say to myself: ‘Wake up! Hold on.’ In this way I can provide encouragement to myself … facing the mirror.
Both patients and caregivers described ways in which optimism, the “joy of life,” “awakening,” belief in God, connectedness to nature, and artistic creativity empowered them. The support provided by informal caregivers – the immediate family circle, friends, internet forums, or complementary medicine practitioners – was greatly appreciated and valued. Informal caregivers emphasized the need for a weekly schedule for visiting, addressing the patient’s sense of loneliness.
Some palliative HCPs and family medicine practitioners emphasized the importance of family support within the context of connectedness, feeling loved, and helping patients maintain dignity. Professionalism and round-the-clock availability of medical treatment at home was reported by patients and informal caregivers, who praised the commitment of the medical team and their common struggle to “win the battle.” At the same time, some patients and informal caregivers expressed a lack of optimal palliative care. They described feeling “neglected,” sometimes even improperly treated (e.g., nonavailability of a psychiatric consultation); often sensing a lack of empathy; frustration with the absence of a medical “solution” for their disease; an often “too practical and cold” team approach; a lack of continuity of care; an expectation that the home treatment was initiated too late; and, in some cases, a feeling that there was a bit of over-treatment (e.g., “no need for the social-worker”). The contrast between praise and criticism of the palliative medical team was addressed in the following patient’s narrative:
While the medical team really tries, they are not always available. What can they do? I feel that I am not receiving adequate treatment … no strengthened … I would like to feel stronger, more treated ….
Some of palliative HCP narratives addressed the difficulty in conducting an open and effective conversation with their patients and informal caregivers about emotional and spiritual concerns:
What’s missing? An open conversation about end-of-life care, without the over-protective involvement of the patient’s partner
Some of the palliative HCP narratives emphasized a “being-doing” approach, while pointing out the restrictions placed by some of the informal caregivers (with “over-doing”), especially with respect to gastrointestinal-related concerns:
The patient’s wife is not cooperating with the palliative care treatment. She is trying to save him … argues with him when he doesn’t want to eat … refuses to let him go …
Many participants from all 4 groups described a reluctance to discuss death and dying, recognizing them as a significant and unaddressed concern. A small number of patients wrote about their imminent death, while asking for more information and options to make it’s the process less prolonged. Informal caregivers also addressed this concern, describing their difficulty in openly talking about death and dying with the patient.
We didn’t know what to do … what to tell her … how to discuss it with her. There was no preparation for the end of life. There was disappointment. No one spoke to us about it … or gave us guidance …
Terms such as “Giving up on life” and “a will to die” were some of the concerns highlighted by family physicians, while hospice HCPs were more concerned with whether or not the patient was aware of the impending death.
Discussion
The differences in how patients, informal caregivers, palliative care HCPs, and family medicine physicians perceive QoL-related concerns among patients in hospice care are to be expected. The quantitative findings of the present study showed that informal caregivers gave higher scores (i.e., greater severity) than patients for fatigue on ESAS (p =0.009); and family physicians lower scores than patients for ESAS drowsiness (p =0.046). Compared with patients, palliative HCPs gave higher scores for patient emotional-spiritual concerns (p =0.02); lower scores for gastrointestinal concerns (p =0.048); and higher scores for overall function (p =0.049).
The quantitative narrative-based analysis identified a sense of unmet needs and expectations among patients and informal caregivers; and frustration and difficulty in sharing emotional and spiritual concerns among palliative HCPs and family physicians. All 4 groups identified the absence of a discussion on and guidance for issues related to death and dying. The findings are in keeping with those of a previous study on patient–caregiver–HCP communication challenges (Reblin et al. Reference Reblin, Clayton and Xu2017), as well as a study examining end-of-life discussions, suggesting a need for coaching HCPs in order to promote communication in advanced palliative care settings (Steven et al. Reference Steven, Lange and Schulz2019). In a similar vein, Bovero et al. emphasized the need to encourage the communicative exchange between and reflective awareness among HCPs through training. This, while exploring perspectives of nurse assistants, nurses, psychologists, and physicians about the sense of dignity in the context of end-of-life care, including emotional and spiritual perspectives (Bovero et al. Reference Bovero, Tosi and Botto2020). At the same time, the finding regarding the discrepancy between palliative HCP and patient scores for emotional-spiritual concerns contrasts with the findings of Kaba et al., with patients and informal caregivers reporting that physical complaints were considered to be far more important than the need for emotional and spiritual support (Kaba et al. Reference Kaba, de Fouw and Deribe2021).
The findings of the present study indicate that informal caregivers are likely to allocate a greater severity of the patient’s fatigue on ESAS than the patients themselves. These findings are similar to those reported in other studies published in the palliative care literature, in which informal caregivers were found to rate patients’ QoL-related burden more severely than the patients themselves (Ishida et al. Reference Ishida, Sato and Komatsu2022). At the same time, these findings should be interpreted with caution, in light of a 1999 Canadian study in which ESAS scores were found to vary greatly among caregivers, nurses, and patients with advanced cancer (Nekolaichuk et al. Reference Nekolaichuk, Maguire and Suarez-Almazor1999). The gap between the expectations of patients/caregivers and palliative HCPs/family physicians needs to be addressed in order to create open discussion and proactively provide guidance for these challenging concerns. Lee and Loiselle proposed a “Temporal Existential Awareness and Meaning Making” model, with the recommendation that existential discussions be considered in any cancer-related setting, and not be deferred to end-of-life care (Lee and Loiselle Reference Lee and Loiselle2012). Grumann and Spiegel interviewed 12 female home hospice patients with advanced cancer, and found that half reported that they were frequently troubled by unresolved issues, with high levels of anxiety and an interest in actively discussing their impending death (Grumann and Spiegel Reference Grumann and Spiegel2003). Zana et al. compared hospice care volunteers to paid employees, and found that fear of death was significantly lower among volunteers, with lower levels of exhaustion and higher levels of psychological well-being (Zana et al. Reference Zana, Kegye and Czeglédi2020). Barnett el al. evaluated 90 hospice nurses and found that a less severe fear of death and death avoidance was associated with a more positive attitude toward the care of the dying patient (Barnett et al. Reference Barnett, Reed and Adams2021). Moreover, a 40-hour Zen Buddhist training program for hospice volunteers was reported to increase compassion and decrease fear of death (Scherwitz et al. Reference Scherwitz, Pullman and McHenry2006). Claxton et al. examined a palliative care volunteer training program, in which participants reported that they were significantly more able to cope with death and dying, though no change was noted on the Collett-Lester Fear of Death Scale (Claxton-Oldfield et al. Reference Claxton-Oldfield, Crain and Claxton-Oldfield2006). Another study found that an educational initiative for palliative HCPs helped positively modify perspectives on death and end-of-life care (Testoni et al. Reference Testoni, Sblano and Palazzo2020). Changes in on their role in end-of-life care were reported in a study of a 3-day course designed for HCPs trained in anthroposophic medicine and integrative oncology (Ben-Arye et al. Reference Ben-Arye, Keshet and Livas2018). This research suggests that emotional, spiritual, and existential concerns are significant across the spectrum of hospice care, particularly for patients and HCPs who need to address their own fears about death and dying.
The present study may provide insights into how HCPs and family physicians can better address emotional-spiritual concerns among their patients and informal caregivers, including the fear of death. It is most likely that palliative HCPs and family physicians would prefer to focus on a “safer” discussion on biophysical concerns such as fatigue, pain, and gastrointestinal symptoms. In light of the insights from the study findings as they relate to communication between oncology HCPs, patients, and informal caregivers, we recommend the creation of training programs for palliative HCPs and family physicians, with the goal of promoting an open and nonjudgmental therapeutic setting, addressing patient’s health beliefs, including spiritual and existential perspectives. This, while discussing unmet needs, expectations, and goals of the Integrative Oncology (IO) and palliative treatment program. Research on such training initiative may provide insight on how to narrow the emotional and spiritual-related communication gap, creating a safe environment in which all participants can engage in a discussion on what may be perceived as taboo or a subject “not to be discussed.” It is advisable that the research plan be accompanied by a medical education intervention, to be designed by a multidisciplinary team of researchers and clinicians, as well as patients, informal caregivers, and advocates. Mixed qualitative and quantitative research methodologies assessing changes in knowledge, attitude, skills, and implementation may enrich the evaluation process. Medical educators may also consider adding role-play and Objective Structured Clinical Examination assessments to the overall training evaluation.
The present study has a number of limitations which preclude reaching any conclusions from the findings and which need to be addressed in future research. The lack of randomization may have potentially led to a selection bias, with the participating patients not representative of the diverse cohort of home hospice care. In addition, the study sample was relatively small and with a low response rate among family physicians, with underrepresentation of nurses and no representation of social workers in the palliative HCP cohort. Other methodological limitations include a lack of follow-up assessment that would enable intragroup analysis exploring changes in symptom severity and interpretation. Future research should incorporate follow-up assessment with a larger sample size, allowing matching of a patient with the other 3 stakeholders, as well as MANOVA procedures. Another significant limitation is the use of a single study interviewer, who despite his linguistic capabilities and cross-cultural background may not have been attuned to all cultural or religious nuances. Future research needs to examine a more diverse and international cohort, with varied social, cultural, and religious characteristics and addressing the unmet concerns of hospice care patients. The research should consider exploring perspectives of other palliative HCPs, such as social workers and integrative oncology practitioners providing care in the home hospice setting.
In summary, the findings of the present study suggest that exploring a multifaceted cohort of home hospice patients, informal caregivers, palliative HCPs, and family physicians may provide insight on how to reduce communication gaps and address unmet needs of patients, particularly regarding emotional and spiritual concerns. Educational initiatives with programs providing training to all 4 groups may help bridge this gap, including with respect to emotional-spiritual concerns during end-of-life care.
Data availability statement
Data transparency is available pending to request from the submitting author.
Acknowledgments
We would like to thank Ms. Ronit Leiba for her assistance in the statistical analysis.
Author contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Eran Ben-Arye, Jamal Dagash, Miri Golan, and Erez Baruch. Analysis were performed by Eran Ben-Arye, Noah Samuels, Yael Keshet, and Jamal Dagash. The first draft of the manuscript was written by Eran Ben-Arye, and Noah Samuels and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
The first and second authors are regarded as co-first author based on their equal contribution to this study.
Funding
No funding was granted for this study.
Competing interests
All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that they have received no support from any organization for the submitted work; have no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; and no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval
The protocol of the study was approved by the Ethics Review Board (Helsinki Committee) at the Clalit Health Services, Israel (research registration COM-14-0058).





 Open access
Open access