


Introduction
Childhood maltreatment has long term impacts on several domains of functioning and would be among the most important risk factors for psychopathology (Teicher et al., Reference Teicher, Gordon and Nemeroff2022). Among mothers, histories of childhood maltreatment have been associated with poorer mental health during the perinatal period (Garon-Bissonnette, Grisé-Bolduc, et al., Reference Garon-Bissonnette, Grisé-Bolduc, Lemieux and Berthelot2022; Racine et al., Reference Racine, Devereaux, Cooke, Eirich, Zhu and Madigan2021) and with insecurities regarding motherhood (Berthelot, Lemieux, et al., Reference Berthelot, Lemieux, Garon-Bissonnette and Muzik2020). Trauma resulting from maltreatment may also interfere with the mother’s ability to respond adequately to her child’s needs (Savage et al., Reference Savage, Tarabulsy, Pearson, Collin-Vezina and Gagne2019), particularly when the child’s behaviors trigger traumatic memories (Schechter, Reference Schechter2019) or when the mother struggles with postpartum psychopathology (Bouvette-Turcot et al., Reference Bouvette-Turcot, Fleming, Unternaehrer, Gonzalez, Atkinson, Gaudreau, Steiner and Meaney2020; Muzik et al., Reference Muzik, Bocknek, Broderick, Richardson, Rosenblum, Thelen and Seng2013). These possible effects of trauma on parental behavior and the documented embedding of trauma in biological systems, which may impact the child through epigenetic mechanisms (Stenz et al., Reference Stenz, Schechter, Serpa and Paoloni-Giacobino2018) and altered placental-fetal stress physiology (Moog et al., Reference Moog, Buss, Entringer, Shahbaba, Gillen, Hobel and Wadhwa2016), may contribute to the higher risk of developmental problems observed in offspring of mothers exposed to childhood maltreatment (Folger et al., Reference Folger, Eismann, Stephenson, Shapiro, Macaluso, Brownrigg and Gillespie2018; Garon-Bissonnette, Duguay, et al., Reference Garon-Bissonnette, Duguay, Lemieux, Dubois-Comtois and Berthelot2022; Letourneau et al., Reference Letourneau, Dewey, Kaplan, Ntanda, Novick, Thomas, Deane, Leung, Pon and Giesbrecht2019). Still, little is known about protective factors that could be efficiently addressed by psychosocial interventions to mitigate the intergenerational transmission of childhood maltreatment (Berthelot, Garon-Bissonnette, et al., Reference Berthelot, Garon-Bissonnette, Lemieux, Drouin-Maziade and Maziade2020).
The degree to which histories of childhood maltreatment interfere with parenthood and the parent-child relationship may partly depend on the extent to which parents have resolved these traumatic experiences (Jacobvitz et al., Reference Jacobvitz, Leon and Hazen2006; Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2003; Swerbenski et al., Reference Swerbenski, Sturge-Apple, Messina, Toth, Rogosch and Cicchetti2023). Four complementary operationalizations of (un)resolved traumas have emerged from attachment research in the last decades. First, Main and Hesse observed that, when questioned about experiences of loss or abuse in the course of the Adult Attachment Interview (AAI), some adults showed brief slips in the monitoring of reasoning and discourse, which have been conceptualized as resulting from interference of dissociated memories with consciousness and cognitive processes or unusual absorptions in painful and distressing memories (Hesse, Reference Hesse, Cassidy and Shaver2008). These unresolved/disorganized (U/d) states of mind were subsequently shown to be associated with maternal frightening or frightened behaviors (Jacobvitz & Reisz, Reference Jacobvitz and Reisz2019) as well as with mother-infant disorganized attachment relationships (Madigan et al., Reference Madigan, Bakermans-Kranenburg, Van Ijzendoorn, Moran, Pederson and Benoit2006).
Second, expressing concerns that U/d states of mind may not properly capture the extent of the distortions in self and other representations manifested by adults who experienced severe and pervasive traumas, such as childhood maltreatment, Lyons-Ruth and colleagues developed the Hostile-Helpless (H/H) coding system (Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2005). As per Main and Hesse’s coding system, Lyons-Ruth’s paradigm uses the AAI, but relies on the entire interview instead of focusing on questions probing about loss or abuse. H/H states of mind are coded when one manifests contradictory and unintegrated emotions regarding an attachment figure whilst identifying with this caregiver (Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2005). H/H states of mind have been associated with dysfunctional parent-child interactions, maltreating parenting behaviors, disorganized mother-infant relationships and child behavior problems (Turgeon et al., Reference Turgeon, Milot, St-Laurent and Dubois-Comtois2022).
Recently, Swerbenski and colleagues (2023) operationalized trauma resolution through a measurement of the degree of acceptance and forgiveness expressed by adults regarding the experiences and circumstances of their childhood upbringing. Their coding system, the Infant and intergenerational relationships coding system (IIRCS; Swerbenski & Sturge-Apple, Reference Swerbenski and Sturge-Apple2020) is applied to the Parent Development Interview and yields a score of acceptance and forgiveness ranging on a scale from 1 to 9. As reported by the authors of the instrument, it is qualitatively distinct from the U/d and H/H coding systems as it yields dimensional scores rather than categories and proposes to capture resilience promoting factors rather than deficits or dysfunctions. Primary results showed that narrative coding of acceptance and forgiveness is only slightly associated with verbal abilities and explains between 2 and 5% of the variance in parenting stress, perception of parenting competence and maternal sensitivity. Small to moderate differences in acceptance and forgiveness were observed between maltreating mothers and non-maltreating mothers. Acceptance and forgiveness was also shown to be negatively associated with depressive symptoms.
Finally, Berthelot and colleagues developed the concept of trauma-specific reflective functioning (T-RF), a measure of the ability to mentalize about experiences of childhood maltreatment and other interpersonal traumas (Berthelot et al., Reference Berthelot, Ensink, Bernazzani, Normandin, Luyten and Fonagy2015). Complementary to U/d and H/H coding systems, which measure alterations in the organization of discourse, T-RF assesses the complexity of thought processes in relation to trauma. T-RF can be coded in relation to any type of interpersonal trauma, including abuse (physical, sexual, emotional), neglect (physical or emotional), domestic violence and other adverse childhood experiences (e.g. bullying, having a parent being unpredictable as a result of a severe mental illness), contrasting with the U/d coding system, which can only be applied to experiences of abuse (Main et al., Reference Main, Goldwyn and Hesse2002), and the H/H coding system, which evaluates attachment representations (Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2005). Interestingly, previous studies showed that the three coding systems would not overlap: no associations were observed between U/d and H-H states of mind (Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2003) nor between U/d states of mind and T-RF (Ensink et al., Reference Ensink, Berthelot, Bernazzani, Normandin and Fonagy2014), suggesting that the three systems assess different and complementary dimensions of the psychological resolution of trauma. Of note, the T-RF coding system shares some similarities with Swerbenski and colleagues’ (2023) system in that both measures aim to identify resilience promoting factors, yield dimensional scores and consider as positive indices of resolution evidence of perspective-taking, self-reflection and recontextualization of past events in the light of developmental acquisitions. However, T-RF captures a broader mode of thinking about trauma and includes several indices of failures to mentalize trauma and of positive trauma resolution that are not captured by the IIRCS, whilst the concept of “forgiveness” (ex. letting go of negative feelings towards the caregiver; improved relationships or attempts to improve relationships with the caregiver; prosocial change towards the caregiver) is unique to the Swerbenski and colleagues’ coding system.
Research on the emerging paradigm of T-RF has been limited so far by the lack of an optimal assessment measure. Indeed, T-RF can only be scored from interview sections directly discussing interpersonal traumas and previous studies used assessment protocols (i.e., the AAI or the Parent Development Interview) that were not specifically designed to enquire about different types and dimensions of trauma. A primary goal of the current study is thus to enable further use of the T-RF coding system by proposing and validating a refined assessment protocol of T-RF.
Mentalizing trauma
Mentalizing trauma refers to the ability to reflect on the psychological and relational impact of trauma and to think of traumatic experiences in a coherent and emotionally grounded fashion. More precisely, a person is considered reflective in relation to trauma when that person (a) is able to identify trauma-related mental states, (b) is conscious that the experience was abusive or neglectful, (c) acknowledges the developmental impact of the traumatic experiences, (d) is aware of the repercussions of trauma in the present (on self, experience of parenthood, parent-child relationship, etc.) or describes coping mechanisms limiting its impact, (e) has a coherent representation of the perpetrator’s mental states, and (f) avoids reenacting the experience of trauma. As for general mentalization abilities (Luyten et al., Reference Luyten, Fonagy, Lowyck, Vermote, Bateman and Fonagy2012), mentalizing trauma involves cognitive and affective ways of approaching traumatic issues. The cognitive dimension of T-RF refers to a process of perspective-taking in relation to trauma, such as looking at one’s own thought and emotional processes from the outside, and trying to figure out others’ mental states underlying their behaviors in the context of trauma. The affective dimension of T-R refers to an interest in making sense of internal experiences whilst accepting and tolerating experiencing unpleasant emotions.
T-RF was originally coded using the questions about childhood abuse from the AAI using an addendum to the existing reflective functioning coding manual specifically elaborated to capture indices of poor and good mentalization in relation to trauma. Recently, the Failure to Mentalize Trauma and Adverse Relationships Questionnaire (FMTQ), a self-report measure of T-RF, was developed to assess different types of failures in the mentalization of past or recent trauma, defined as indications that the respondent is not able to maintain coherent thinking when discussing these situations and/or indices of definite distortions in the perception of the impact of trauma on the self, on mental states, and on behaviors (Berthelot et al., Reference Berthelot, Savard, Lemieux, Garon-Bissonnette, Ensink and Godbout2022). The FMTQ is different from the T-RF coding system in that it measures indices at the lower spectrum of the T-RF scale, but does not capture the complexity of thought processes in relation to trauma.
The ability to mentalize about past trauma emerged as an important psychological determinant of resilience and adaptation in mothers exposed to childhood maltreatment, as supported by four sets of findings. First, in pregnant women with histories of abuse and neglect, high T-RF, assessed using the T-RF scale applied to the AAI, was associated with a positive investment in pregnancy and with the quality of couple functioning (Ensink et al., Reference Ensink, Berthelot, Bernazzani, Normandin and Fonagy2014). Second, T-RF prospectively predicted infant attachment disorganization at 18-months postpartum over the effect of U/d states of mind and general mentalization abilities (Berthelot et al., Reference Berthelot, Ensink, Bernazzani, Normandin, Luyten and Fonagy2015). Third, in sexually abused mothers, good mentalization abilities in relation to these experiences, assessed using the T-RF scale applied to the PDI, were shown to act as a buffer in the intergenerational cycles of sexual abuse (Borelli et al., Reference Borelli, Cohen, Pettit, Normandin, Target, Fonagy and Ensink2019). Fourth, in adult community samples, impairments in mentalizing trauma and adverse relationships, measured using the FMTQ, were shown to be associated with greater psychiatric symptoms, including anxio-depressive, post-traumatic and dissociative symptoms as well as personality dysfunctions (Berthelot & Garon-Bissonnette, Reference Berthelot and Garon-Bissonnette2024; Berthelot et al., Reference Berthelot, Savard, Lemieux, Garon-Bissonnette, Ensink and Godbout2022; Gamache et al., Reference Gamache, Savard, Lemieux and Berthelot2021). These preliminary findings call for further development and operationalization of the concept of T-RF.
Coding T-RF using the trauma meaning-making interview
Recent work on trauma processing used an interview especially focusing on childhood maltreatment, the Trauma Meaning-Making Interview (Simon et al., Reference Simon, Kobielski and Feiring2006), to better understand the different strategies developed by youths and adults to make meaning of trauma. This interview has the advantage of being relatively brief and of delving into multiple dimensions of trauma, such as the experience of trauma, the thoughts and feelings about the trauma, its discovery at the time it happened as well as over time, and the perceived effects of trauma (Simon et al., Reference Simon, Feiring and Kobielski McElroy2010). To date, this interview is coded using a system developed to capture three strategies used by youths and adults for processing potentially traumatic events: Constructive, Absorbed and Avoidant strategies. These strategies are grounded in theory and research on the ways individuals differentially employ approach and avoidance strategies to regulate attention to trauma-related memories, cognitions, and emotions (Brewin et al., Reference Brewin, Dalgleish and Joseph1996; Ehlers & Clark, Reference Ehlers and Clark2000; Holmes, Reference Holmes1996; Horowitz, Reference Horowitz1986). Similar to the coding of attachment representations using the AAI, the TMMI coding uses a structural approach that considers both the content and manner of speakers’ discourse. However, the TMMI coding focuses on discourse around traumatic events and their sequelae whereas the AAI coding centers on the processing of attachment experiences.
Those with Constructive processing strategies generally provide clear descriptions of traumatic experiences during the interview, are actively involved in trying to make meaning of their experiences and are inclined to revise their perception in the face of changing circumstances. While seeing the trauma as belonging to the past, they remain engaged in thinking about its significance for past and current functioning (Simon et al., 2006, 2010). In contrast, Absorbed speakers seem to be overwhelmed by abuse-related mental states, which leads to difficulties in discerning key information from which to construct useful meanings. These participants actively attempt to make sense of trauma but this remains unproductive and lacks insight (Simon et al., 2006, 2010). Finally, Avoidant speakers actively distance themselves from trauma, avoid getting emotionally engaged in the task, minimize traumatic experiences, and deny feelings of vulnerability (Simon et al., 2006, 2010). To capture unresolved trauma processing, participants were also assigned to a secondary classification of Unresolved/disorganized trauma by applying Main and colleagues coding systems for traumatic discourse (Main et al., Reference Main, Goldwyn and Hesse2002). Previous studies supported the validity of this classification system by showing that abuse stigmatization, post-traumatic stress disorder (PTSD) symptoms, and negative reactions from others predicted trauma-processing classification more than six years following sexual abuse (Simon et al., Reference Simon, Feiring and Cleland2016), and by showing distinctive associations between trauma-processing strategies, psychopathological symptoms and sexual problems (Simon et al., Reference Simon, Feiring and Kobielski McElroy2010).
The TMMI is particularly well-suited to assess T-RF. Indeed, it focuses on interpersonal trauma, allows one to probe for different types of trauma (e.g., sexual abuse, domestic violence, parental neglect, and peer bullying) and covers complementary dimensions of traumatic experiences of important concern for the coding of T-RF (e.g., experience of trauma; experience of disclosure; perceived effects). In addition, the fact that this interview can also be coded for trauma-processing strategies offers the occasion to evaluate the construct validity of the T-RF coding system.
Trauma, reflective functioning and psychological understanding of the child
In the last decades, Fraiberg’s observation that traumatic experiences from the past may invade the mother-infant relationship by altering mothers’ representation of the child (Fraiberg et al., Reference Fraiberg, Adelson and Shapiro1975) found strong support in two sets of findings. First, empirical research documented a higher risk of bonding and attachment disturbances with their infants in mothers who experienced trauma (Erickson et al., Reference Erickson, Julian and Muzik2019; Vaillancourt et al., Reference Vaillancourt, Pawlby and Fearon2017). Second, the ability of mothers to understand the psychological experience of their child has been shown to buffer the impact of childhood trauma on parenting behaviors. For instance, studies using the parental reflective functioning scale applied to the Parent Development Interview (PDI; Slade et al., 2003, 2005), a coding system especially developed to inform about how parents reflect upon the psychological world of their child and upon their own parental experience, showed that parental reflective functioning was positively associated with maternal sensitivity (Alvarez-Monjarás et al., Reference Alvarez-Monjarás, McMahon and Suchman2019; Stacks et al., Reference Stacks, Muzik, Wong, Beeghly, Huth-Bocks, Irwin and Rosenblum2014; Suardi et al., Reference Suardi, Moser, Sancho Rossignol, Manini, Vital, Merminod, Kreis, Ansermet, Rusconi Serpa and Schechter2020) as well as mother-infant attachment in community samples of mothers (Camoirano, Reference Camoirano2017) and in mothers exposed to childhood maltreatment (Ensink et al., Reference Ensink, Normandin, Target, Fonagy, Sabourin and Berthelot2015; Huth-Bocks et al., Reference Huth-Bocks, Muzik, Beeghly, Earls and Stacks2014; Schechter et al., Reference Schechter, Coots, Zeanah, Davies, Coates, Trabka, Marshall, Liebowitz and Myers2005). Similar results were found with another measure using video segments of mother-infant interactions, the Insightfulness Assessment (Oppenheim et al., Reference Oppenheim, Koren-Karie and Sagi2001). Indeed, mothers who experienced sexual abuse during their childhood were shown to be generally less insightful regarding their children’s internal states than mothers who did not experience such traumas (Koren-Karie & Getzler-Yosef, Reference Koren-Karie and Getzler-Yosef2019), and mothers classified as insightful were more likely to be sensitive in their interactions with their infants and to have securely attached children (Koren-Karie et al., Reference Koren-Karie, Oppenheim, Dolev, Sher and Etzion-Carasso2002).
Although there is no doubt that maternal insightfulness and maternal reflective functioning have positive implications for the parent-infant relationship and for the development of the child, still little is known about the determinants of these abilities, especially in survivors of childhood maltreatment (Koren-Karie & Getzler-Yosef, Reference Koren-Karie and Getzler-Yosef2019). Further research is particularly required with this population considering that empirical evidence suggest that the determinants of psychopathology and reflective functioning would be different among adults with histories of childhood maltreatment than among adults who did not face such adverse life events (Nemeroff et al., Reference Nemeroff, Heim, Thase, Klein, Rush, Schatzberg, Ninan, McCullough, Weiss, Dunner, Rothbaum, Kornstein, Keitner and Keller2003; Teicher et al., Reference Teicher, Gordon and Nemeroff2022; Teicher & Samson, Reference Teicher and Samson2013). For instance, Moser et al. (Reference Moser, Suardi, Rossignol, Vital, Manini, Serpa and Schechter2019) observed that parental reflective functioning was positively associated with brain activation in the ventromedial prefrontal cortex, and negatively associated with activation in the dorsolateral prefrontal cortex and the insula in mothers without history of trauma when they watched scenes of separation with their toddler, whereas such associations were not observed in mothers with histories of child abuse. The determinants of parental behaviors may also be different in trauma-exposed and non-exposed parents, as suggests previous evidence showing that, in mothers who experienced trauma, it is not the absence of attachment-related mentalization that is the most important for predicting the quality of the mother-infant relationship, but more specifically how they mentalize regarding trauma (Berthelot et al., Reference Berthelot, Ensink, Bernazzani, Normandin, Luyten and Fonagy2015). The current study thus aims to evaluate the association between T-RF and parental reflective functioning (PRF) as well as the association between both types of mentalization (PRF and T-RF) and maternal insightfulness in mothers who experienced childhood trauma.
Present study
The aim of the present study is to validate the Trauma-specific reflective functioning scale applied to the Trauma Meaning-Making Interview by (1) describing score distributions, inter-rater reliability, internal consistency and association with the characteristics of trauma, (2) evaluating the associations with related measures of trauma processing and maternal reflective functioning, (3) assessing the association with internalized psychopathology (depression and PTSD), and (4) evaluating whether T-RF offers a unique contribution to maternal insightfulness. Based on previous findings (Ensink et al., Reference Ensink, Berthelot, Bernazzani, Normandin and Fonagy2014), our first hypothesis is that T-RF will be independent from the characteristics of trauma but will be associated with sociodemographic characteristics. A second hypothesis is that moderate-size associations will be observed between T-RF and maternal RF after controlling for the effect of potential confounders. A third hypothesis is that mothers with constructive trauma-processing strategies will show better mentalization in relation to trauma than mothers with Avoidant, Absorbed or Unresolved/Disorganized strategies, but that the correlations between T-RF and the four scales of trauma-processing will be modest. Accordingly, we expect participants classified as Constructive to show higher T-RF than participants classified as Avoidant or Absorbed, and participants classified as Organized to show higher T-RF than participants classified as Unresolved/Disorganized. As suggested by previous research documenting an association between psychiatric symptoms and self-reported failures in the mentalization of trauma (Berthelot & Garon-Bissonnette, Reference Berthelot and Garon-Bissonnette2024; Berthelot et al, Reference Berthelot, Savard, Lemieux, Garon-Bissonnette, Ensink and Godbout2022), a fourth hypothesis is that T-RF and trauma-processing strategies will be negatively associated with symptoms of PTSD and depression. Finally, our fifth hypothesis is that mothers with good T-RF will be more likely to be classified as Positively insightful at the Insightfulness Assessment than mothers with poor or limited T-RF, the latter being more likely to be classified as non-insightful with regards to their child’s emotional experience (i.e., to be classified as one-sided, disengaged or mixed). In addition, we expect T-RF to be associated with dimensions of maternal insightfulness over and beyond the effect of parental mentalization, constructive trauma-processing strategies, maternal education and sociodemographic risk factors.
Methods
Participants and procedure
Participants were 112 women and their infants from a larger longitudinal study (Maternal Anxiety during the Childbearing Years; MACY study; NIH MH080147, PI: Muzik) conducted between 2008 and 2012 and evaluating the effects of childhood maltreatment on postpartum psychosocial adaptation, motherhood and child developmental trajectories. Various recruitment strategies (i.e., invitations during antenatal visits, community advertisements) were used to reach women in pregnancy and up to 4 months postpartum who self-identified as having experienced a “challenging upbringing”. Interested women provided their contact information and were subsequently reached by the research team. Participants first completed a phone interview at 4 months postpartum, followed by two home visits when infants were 6 and 16 months old. Inclusion criteria were being English-speaking, 18 years or older, free of psychosis or active substance use and not reporting any major medical or developmental condition. The study protocol has been described in more detail multiple times (Menke et al., Reference Menke, Morelen, Simon, Rosenblum and Muzik2018; Stacks et al., Reference Stacks, Muzik, Wong, Beeghly, Huth-Bocks, Irwin and Rosenblum2014). The study was approved by our universities’ Institutional Review Boards.
The 112 mothers reported having been exposed to childhood maltreatment at recruitment according to the Childhood Trauma Questionnaire (Bernstein et al., Reference Bernstein, Stein, Newcomb, Walker, Pogge, Ahluvalia, Stokes, Handelsman, Medrano, Desmond and Zule2003). Trauma was reassessed at 6-month postpartum using the Trauma History Checklist (see Measures). As shown in Table 1, all types of traumas were frequent in the sample, and the vast majority of women reported cumulative and chronic trauma. The majority of women were in a relationship with the birth father, employed, and had some post high-school education. However, half of participants reported at least one sociodemographic risk factor among not having a high-school diploma, having an annual income of less than $25,000, being under the age of 22, being a single parent, and belonging to a racial minority.
Participants’ sociodemographic and trauma characteristics
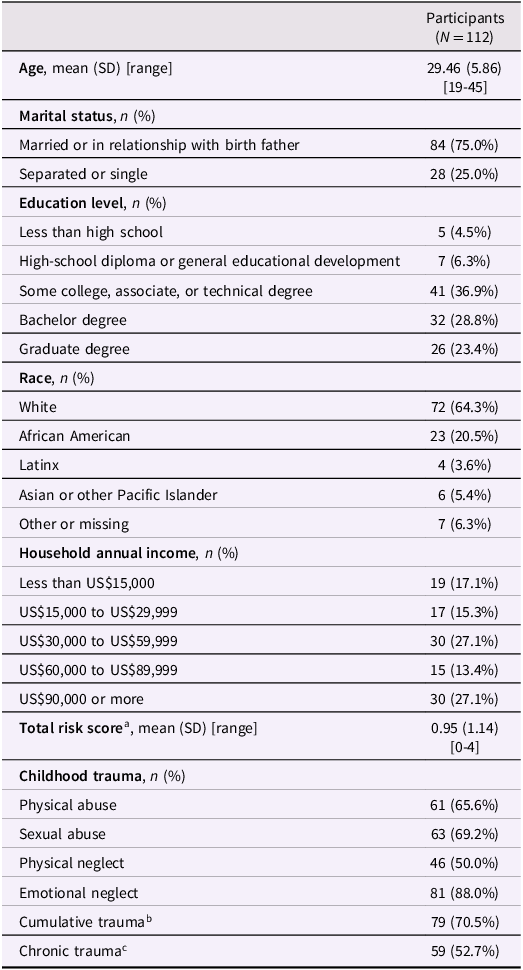
Note.a A risk index was created on a scale of 0 to 4 by adding binary scores (absent vs present) on four recognized risk factors: having an annual income of less than $25,000, being under the age of 22, being a single parent, and belonging to a racial minority; b Cumulative trauma refers to participants having been exposed to two or more types of traumas during childhood; c Chronic trauma is defined as extending over at least two developmental periods (0-5 years; 6–11 years; 12–16 years).
Measures
Interviews
1. Trauma History Checklist. Childhood maltreatment was assessed at 6-month postnatal using the Trauma History Checklist, an instrument described in previous reports (Menke et al., Reference Menke, Morelen, Simon, Rosenblum and Muzik2018). Participants reported on type, frequency, duration, and perpetrator identity for all experiences of childhood maltreatment before 16 years old.
2. Trauma Meaning-Making Interview. Trauma-processing strategies and T-RF were coded from the Trauma Meaning-Making Interview (TMMI), a semi-structured interview developed to assess representations of experiences of childhood maltreatment in youth and adult populations (Simon et al., Reference Simon, Kobielski and Feiring2008). The interview probes about the specific types of trauma that participants considered having been the most distressing and invites participants to provide some details about their experience, to describe their thoughts and feelings when trauma was occurring and over time, to explain whether they disclosed the situation to other people and how they and others reacted, to formulate an understanding concerning some of the reasons why these experiences may have happened, to describe the perceived repercussions of trauma during childhood/adolescence and over time, and to explain how they coped with this experience. Participants were free to provide as many or as few details they wanted during the interview. The interviews, averaging about 30 minutes, were administered at 6-month postpartum and were audio recorded and subsequently transcribed for coding.
Two coding strategies were applied to the TMMI. First, one team of coders evaluated participants’ trauma-processing strategies using a coding system that indexes individual differences in unconscious and semiconscious patterns of regulating attention to trauma-related memories, cognitions, and emotions. Secondly, the narratives were coded by an independent team on trauma-specific reflective capacity (T-RF) tapping into meaning-making, mentalization and reflection based on work on reflective functioning by Peter Fonagy and colleagues (1998). In the following paragraphs we are providing details on coding for the two systems.
Trauma Narrative Coding - Trauma-processing strategies. TMMI verbatims were first coded for trauma-processing strategies (Constructive, Absorbed, Avoidant, Disorganized) by two trained and certified coders (the developer of the trauma-processing coding system and a trained graduate student) blind to other measures and to the hypotheses of this study. The primary features used in coding is the discourse of the narrative, that is, “how” the participant conveys their experiences (e.g., willingness and ability to evaluate the past from a present-day perspective; coherence). Coders first used a 9-point scale to rate the presence and strength of each processing strategy in a given transcript. Higher scores reflect a stronger and more pervasive use of that strategy. Next, the coder used the constellation of processing style scale scores along with the narrative’s fit to the overall descriptions of the three processing strategies to determine the primary processing strategy and whether a Disorganized sub-classification was warranted. Coders had previously trained and established reliability on two prior samples of TMMI transcripts (Simon et al., Reference Simon, Kobielski and Feiring2006). Prior to that, coders were trained and certified in the codification of attachment using the AAI coding system and used Main and colleagues criteria (2002) to evaluate disorganized processing strategies. Good indications of reliability were obtained for scale scores and classifications of trauma-processing strategies. Intraclass correlation estimates for the continuous scale scores, based on a consistency-agreement, two-way random effects model ranged from .947 to .976, all ps < .001. Inter-rater agreement on the trauma-processing classifications was also strong (κ = .91, p < .001). Disagreements on scale scores of two or more points or on trauma-processing strategy classification were resolved by consensus. Twelve narratives were not coded and were excluded from analyses because the experience described did not meet the traditional legal or psychological criteria for maltreatment. For example, one participant indicated that she experienced neglect as a child but described an incident when her mother left her in alternate care while at work. The analyses on trauma-processing strategies thus included 100 participants.
Trauma Narrative Coding – Trauma-Specific Reflecting Functioning Scale. The ability to mentalize about past trauma was coded from the TMMI using the Trauma-Specific Reflective Functioning Coding System (Berthelot & Garon-Bissonnette, Reference Berthelot and Garon-Bissonnette2023). This measure includes 20 indicators of moderate to high T-RF grouped according to four core dimensions of reflective functions described in Fonagy’s et al., (Reference Fonagy, Target, Steele and Steele1998) original coding system: a) Awareness of the nature of mental states; b) Explicit effort to tease out mental states underlying behavior; c) Developmental aspects of mental states; d) Mental states in relation to the interviewer. Like the traditional RF coding system, the T-RF scale ranges from −1 (refusal to engage in T-RF, bizarre discourse and/or hostility towards the interviewer) to 9 (remarkable and exceptional RF), a score of 5 reflecting a basic understanding of how trauma-related mental states influence behaviors, relationships and current functioning. Two coders (1st and 2nd authors) trained and certified on the Reflective Functioning Scale (Fonagy et al., Reference Fonagy, Target, Steele and Steele1998) independently coded the transcripts
3. Parent Development Interview. To tap into the mothers’ ability to reflect upon their children’s mental states as well as their own mental states when interacting with their child we used the Parent Development Interview-Revised Short Form (PDI; Slade et al., Reference Slade, Aber, Berger, Bresgi and K.2003) at 16-month postpartum. This 30-question semi-structured interview was audio recorded, transcribed and subsequently coded for parental reflective functioning using the Addendum to the Reflective Functioning Coding Manual for Use with the Parent Development Interview (Slade et al., Reference Slade, Bernbach, Grienenberger, Levy and Locker2005).
Parent Development Interview Coding. An independent team of coders had coded the PDI interviews (Slade et al., Reference Slade, Aber, Berger, Bresgi and K.2003) using the Reflective Functioning Coding Manual for Use with the Parent Development Interview (Slade et al., Reference Slade, Bernbach, Grienenberger, Levy and Locker2005). Like the other coding systems of RF, responses during the PDI are scored on a scale ranging from −1 to 9, higher scores indicating higher sophistication of parental reflective functioning. Two trained and reliable coders scored the interviews, and 36% were double-coded. Strong agreement between coders was attained (single measure ICC = 0.76). This coding had been completed in the past and complete description of use of PDI and coding is published in Stacks and colleagues (2014).
4. Insightfulness Assessment (IA) Interview. The capacity of mothers to consider the motives underlying their children’s behaviors and emotional experiences in a positive and child-focused manner (i.e., maternal insightfulness) was assessed at the 6-month home visit using the Insightfulness Assessment (IA; Koren-Karie et al., Reference Koren-Karie, Oppenheim, Dolev, Sher and Etzion-Carasso2002). Mothers were asked to watch three clips from a mother-infant interactive task previously videotaped. After each clip, they were asked about their children’s thoughts and feelings in an audiotaped semi-structured interview. Throughout the interview, mothers were asked for examples from their everyday life that supported their statements. The interviews were subsequently transcribed for coding.
Insightfulness Assessment coding. Coding was performed by one of the co-developers of the IA blind to other measures and to the hypotheses of this study. The classification score (positively insightful, one-sided, disengaged, or mixed), the dichotomous score (insightful or non-insightful) and the continuous scores on the ten dimensions of maternal insightfulness (insight into child’s motives, coherence of thought, complexity in description of child, acceptance, richness of description of child, openness, separateness from child, maintenance of focus on child, worry, and anger) were used in the present study. Extensive description of use and coding of the IA interview in this sample is published in Martinez-Torteya et al. (Reference Martinez-Torteya, Rosenblum, Beeghly, Oppenheim, Koren-Karie and Muzik2018).
Self-report surveys
5. Sociodemographic risk index. During the 6-month home visit, mothers reported on their current relationship status, race, age, education level, and their family’s total annual income. A cumulative risk score was obtained for each mother by assigning a point for the presence of four demographic risk factors (single parent, racial minority status, annual income less than $25,000, and age 22 or younger), and then summing the risk points. Scores in this sample ranged from 0 to 4 (M = 0.95, SD = 1.14).
6. Symptoms of post-traumatic stress disorder (PTSD). Current post-traumatic stress symptoms were measured using the National Women’s Study PTSD Module (NWS-PTSD; Kilpatrick et al., Reference Kilpatrick, Resnick, Saunders and Best1989) administered at the 6-month home visit. This 26-item instrument is a version of the Diagnostic Interview Schedule that was modified for use in large epidemiological studies. The scale items assess all three PTSD domains (intrusion, avoidance, and hyperarousal), and an algorithm follows DSM-IV criteria to derive a PTSD diagnosis (must meet at least 1 intrusion, 3 avoidance, and 2 hyperarousal symptoms). External validity is good, as shown by adequate agreement (kappa = .77) with a clinician-administered structured interview (SCID), high sensitivity of 0.99 and adequate specificity of 0.79, as compared with the SCID (Resnick et al., Reference Resnick, Kilpatrick, Dansky, Saunders and Best1993). A continuous current PTSD symptom count score was used in statistical analyses. PTSD scores ranged from 0 to 17 in this sample (M = 5.85, SD = 4.54) and 38% reached the clinical cutoff for a probable post-traumatic stress disorder.
7. Postpartum Depression Screening Scale. The current depressive symptoms of mothers were measured using the Postpartum Depression Screening Scale (Beck & Gable, Reference Beck and Gable2002) at the 6-month home visit. The PDSS includes 35 items rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate more symptoms of depression (clinical cutoff ≥ 80; Beck & Gable, Reference Beck and Gable2000). In this study, Cronbach’s alpha was α = .96. Depression scores ranged from 35 to 132 in this sample (M = 67.85, SD = 24.39) and 28% reached the clinical cutoff for a probable major depressive disorder.
Data analysis strategy
In the first step, we reported on the psychometric properties of the Trauma-RF scale. Internal consistency was assessed using T-RF scores obtained from the five sections of the TMMI. Intraclass correlations were performed to evaluate inter-rater reliability on a set of 24 transcripts (21% of the sample) coded by the developer of the coding system and a trained Ph.D. student having previous training on the traditional RF coding system. We also evaluated the association between T-RF scores and sociodemographic variables as well as the characteristics of trauma using Pearson correlations for continuous scores and an analysis of variance for categorical variables.
In the second step, we evaluated construct validity by using related measures of trauma-processing (trauma-processing strategies coded from the TMMI), and reflective functioning (parental RF coded from the PDI) using partial correlations for continuous scores and analyses of covariance (ANCOVA) for categorical variables controlling for the effect of confounding variables. We also evaluated whether scores at the T-RF scale correlated with the severity of concurrent depressive and PTSD symptoms using partial correlations.
In the third step, we evaluated whether T-RF was associated with an observational measure of maternal sensitivity to infant internal states (i.e., mothers’ insightfulness). A chi-square analysis was first used to evaluate whether classification on the Insightfulness assessment was homogeneous across participants with poor (−1 to 2), limited (3-4) and good T-RF (≥ 5) and calculated the odds ratios of being classified as positively insightful at the Insightfulness assessment in women with good T-RF in comparison to women with poor or limited T-RF. We next performed multiple regression analyses to evaluate whether T-RF was associated with dimensions of maternal insightfulness over and above the effect of parental RF, trauma-processing (constructive score), and sociodemographic risk factors. For this analysis, we first conducted a factor analysis with Varimax rotation on the 10 subscales of the Insightfulness assessment in order to reduce the number of meaningful variables to be analyzed (see Results and STable 1 in the electronic supplement). A strong factorial structure was obtained and factor scores were used as criteria in the regression models.
Results
Psychometric properties and association with sociodemographic risk factors and the characteristics of trauma
The total scores on the T-RF scale were normally distributed and ranged from −1 to 8, with a mean (3.83, SD = 1.87) and a median (4.00) at the middle point of the scale (4.00). Means on the five subscales ranged from 2.86 to 4.29 (STable 2 in the electronic supplement), revealing that some domains (e.g., how one successfully coped with trauma) may be harder to mentalize than others. The scale showed excellent internal consistency (Cronbach’s α = .92) and removal of any of the subscales did not improve internal consistency. Inter-rater reliability on 24 narratives was excellent (ICC = 0.98 for the global score, 95% CI [.93–.99], and between 0.90 and 0.98 for the five sections of the TMMI).
The complexity of thought processes in relation to trauma was negatively correlated with the sociodemographic risk index and positively correlated with maternal education (Table 2). Scores on the T-RF scale were not significantly associated with transcript lengths, here used as a proxy for verbal abilities. Further analyses thus controlled for the effect of education and sociodemographic risk. T-RF scores were not different in mothers with single trauma (M = 3.43, SD = 1.75) and cumulative trauma (M = 3.96, SD = 1.88), t(89) = −0.22, p = .82, and were not associated with the primary type of trauma (sexual abuse, physical abuse, emotional abuse or neglect), F(3, 91) = 0.59, p = .62, the developmental period at onset, F(6, 83) = 0.49, p = .81, or the persistence of trauma across developmental periods, F(1, 88) = 0.13, p = .72.
Pearson correlations between T-RF, sociodemographic risk, length of TMMI transcripts, internalized problems, maternal reflective functioning and trauma-processing strategies
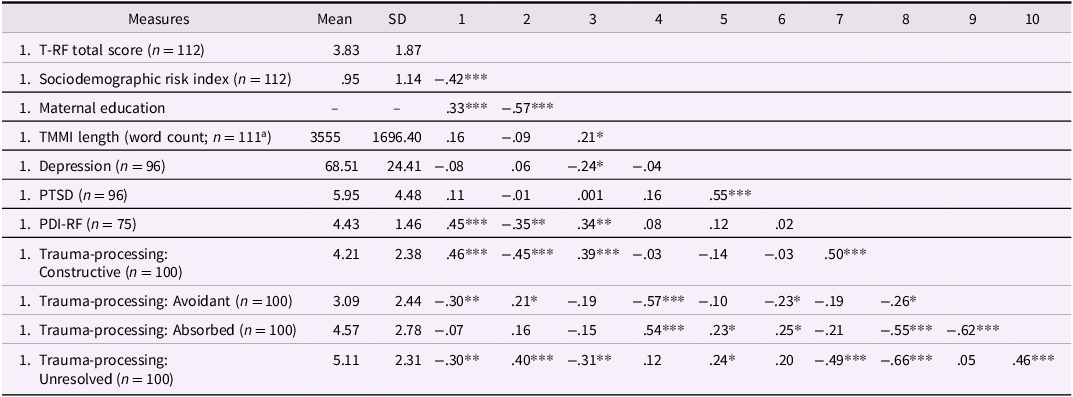
Abbreviations. T-RF = trauma-specific reflective functioning; SD = standard deviation; TMMI = Trauma Meaning-Making Interview. a One outlier was excluded. * p < .05. ** p < .01. *** p < .001.
Association of T-RF with maternal reflective functioning, trauma processing or mental health
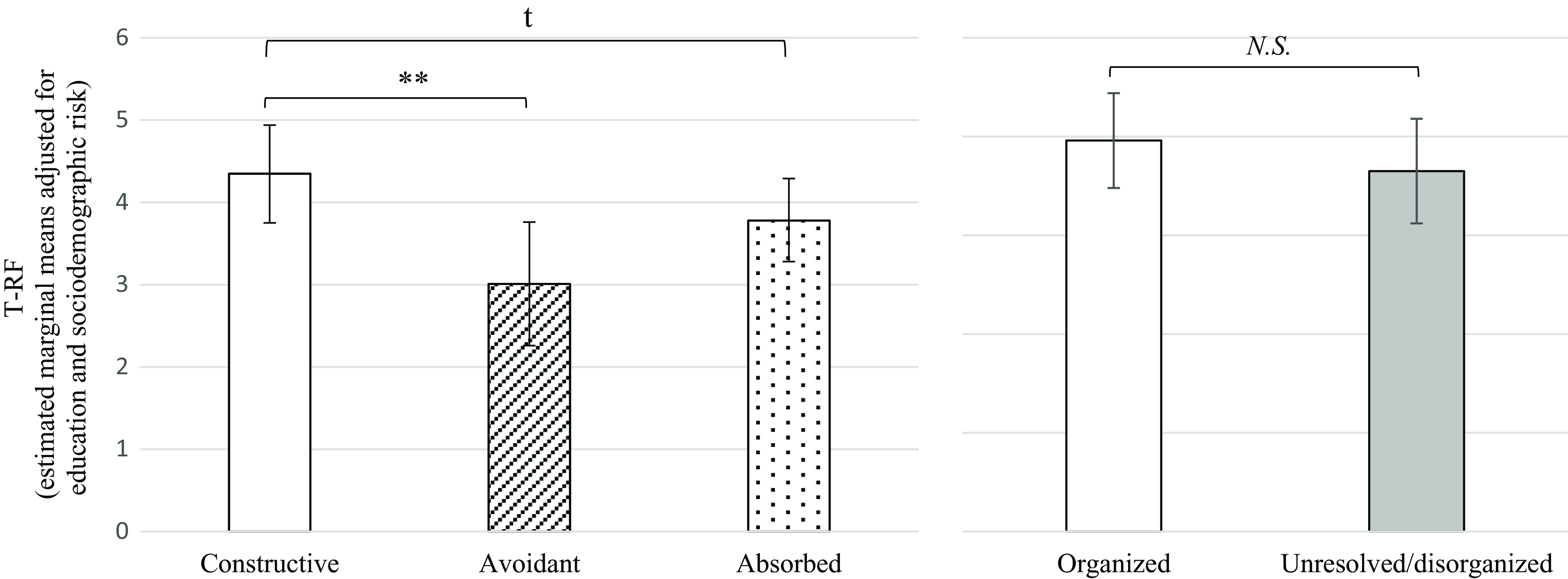
First, partial correlations controlling for maternal education and sociodemographic risk revealed a moderate association (r = .33, p = .005) between the complexity of thoughts regarding trauma (T-RF) and the ability to think of the infant and the mother-infant relationship in terms of internal mental states (parental RF). Second, T-RF scores were positively correlated with the complexity of constructive trauma-processing strategies (r = .30, p = .003) and negatively correlated with the severity of avoidance (r = .22, p = .03) strategy after controlling for the effect of sociodemographic risk and maternal education. Results of an ANCOVA (Figure 1) showed that mothers classified as Constructive had better T-RF than mothers classified as Avoidant and marginally better scores than Absorbed participants. However, mothers classified as Disorganized/unresolved at the TMMI did not have significantly lower T-RF than mothers having an organized narrative. Third, scores on the T-RF coding system were not associated with concurrent depressive and post-traumatic symptoms (Table 2). However, partial correlations controlling for maternal education and sociodemographic risk revealed that avoidant trauma-processing strategies were negatively associated with PTSD symptoms (r = −.23, p = .04) and that absorbed strategies were positively associated with PTSD symptoms (r = .25, p = .03) and marginally associated with depressive (r = .22, p = .05) symptoms.
Trauma-specific mentalization according to categories of trauma-processing strategies. On the left panel, participants T-RF scores were compared across participants classified as having a constructive, avoidant or absorbed narrative when discussing trauma. An ANCOVA controlling for maternal education and sociodemographic risk revealed significant group differences, F(2, 94) = 3.50, p = .03. Contrast analyses showed that participants displaying constructive trauma-processing strategies had significantly higher T-RF than participants with avoidant strategies. On the right panel, the same participants were further classified as displaying organized or unresolved/disorganized states of mind, based on the presence of significant indices of disorganization in the monitoring of discourse and reasoning during the interview. An ANCOVA controlling for maternal education and sociodemographic risk revealed no significant group differences, F(1, 95) = 0.69, p = .41. Error bars represent 95% confidence intervals. T-RF = trauma-specific reflective functioning; N.S. = non significant; ** p ≤ .01. t p ≤ .10.
Contribution of T-RF to maternal insightfulness
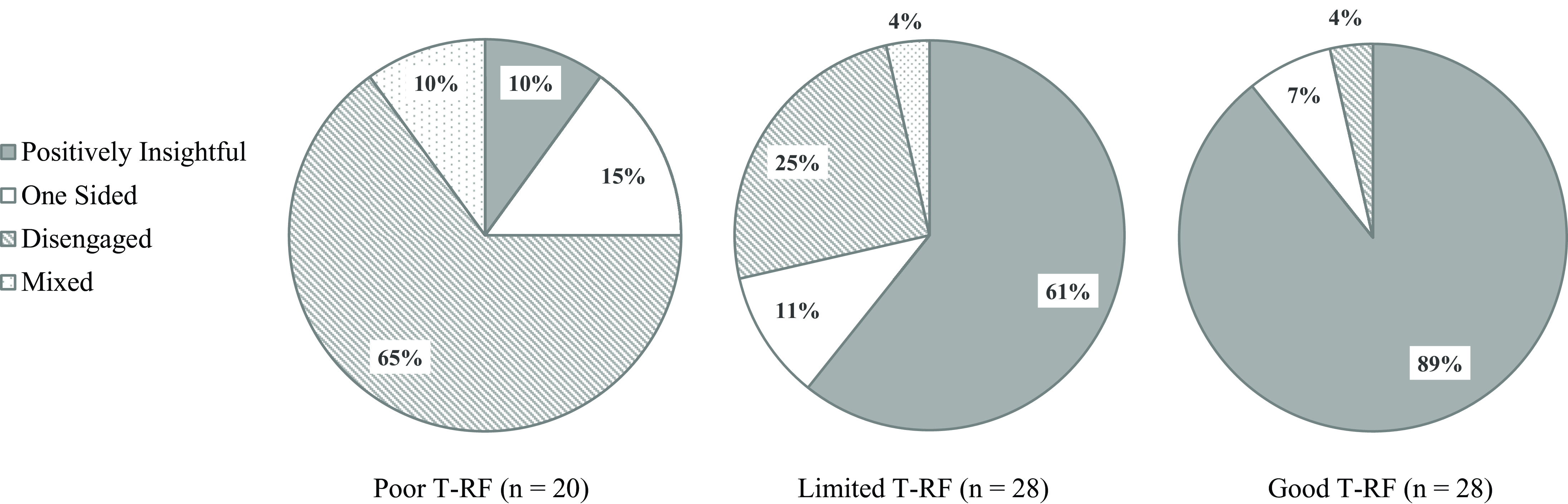
Chi-square analyses showed that classification as Positively Insightful vs non-insightful (i.e. one-sided, disengaged or mixed) was not homogeneous across participants with poor (−1 to 2), limited (3-4) or good T-RF (≥ 5), χ2 = 30.23, p < .001. As shown in Figure 2, mothers with good mentalization abilities with regard to trauma were disproportionately more likely to be classified as positively insightful at the Insightfulness assessment than mothers with poor T-RF (OR = 75.00, 95% CI [11.34–495.95]) and mothers with limited T-RF (OR = 5.39, 95% CI [1.31–22.25]). Mothers who showed distinctive failure in making sense of their traumatic past (i.e., mothers with poor T-RF) were mainly disengaged (65%) during the task and only 10% were classified as insightful regarding their infant internal states. Contrarily, 89% of mothers with good T-RF were positively engaged during the Insightfulness interview. We verified whether this association could be explained by an underlying inability to think in mental state terms (alexithymia) in participants with poor T-RF by contrasting parental reflective functioning scores in mothers classified as positively insightful vs non-insightful. Mothers with low insightfulness had only slightly lower (d = 0.66) parental RF scores on the PDI (M = 4.04, SD = 1.48) than mothers with good insightfulness (M = 4.94, SD = 1.25), t(59) = 2.59, p = .01.
Insightfulness classification according to the level of trauma-specific reflective functioning. T-RF was coded blind to insightfulness classification. Poor T-RF was defined as a score between -1 and 2, limited T-RF was defined as a score of 3 or 4, and good T-RF was defined as a score ≥ 5, as in previous studies (Berthelot et al., Reference Berthelot, Ensink, Bernazzani, Normandin, Luyten and Fonagy2015). Chi-square analyses showed that mothers’ classification as positively insightful vs non-insightful (i.e. one-sided, disengaged or mixed) was not homogeneous across participants with poor, limited or good T-RF, χ2 = 30.23, p < .001. T-RF = trauma-specific reflective functioning.
We finally evaluated whether T-RF was associated with dimensions of maternal insightfulness over and above the effect of parental RF, trauma-processing (constructive score), maternal education and sociodemographic risk factors. The factor analysis of the 10 subscales of the Insightfulness assessment yielded a strong three-factor structure explaining respectively 56, 22 and 8% of the total variance (STable 2 in the electronic supplement). Factor 1 reflected a positive and complex engagement in the task and was composed of the complexity, insight, acceptance, openness, richness and coherence subscales. Factor 2 was capturing an ability to stay focused on the child and on the task, without being overly distracted by concerns, and was composed of the focus, worry (negative loading) and separateness subscales. The last factor was composed of the anger subscale alone. For this factor, we thus used the original subscale score rather than the factor score. Multiple regression analyses (Table 3) showed that only T-RF (p = .007) was significantly associated with positive insightfulness (Factor 1), no predictors were associated with the quality of the engagement in the task (Factor 2) and only T-RF (p = .028) was associated with anger. Results are presented in Table 3.
Multiple regressions assessing the association between T-RF, constructive trauma-processing strategies, parental reflective functioning, maternal education, sociodemographic risk and the three dimensions of insightfulness
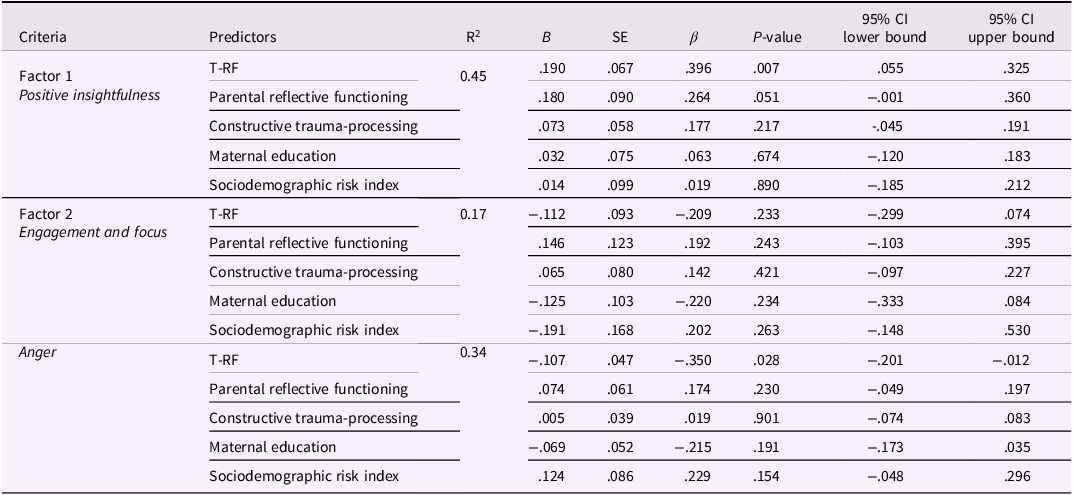
A factor analysis with Varimax rotation was performed to regroup the ten subscales into a limited number of meaningful clusters (see STable 2). Three multiple regressions were next performed with T-RF, constructive trauma-processing strategies, parental reflective functioning, and sociodemographic risk as predictors and the factor scores as criteria. Abbreviations. T-RF = trauma-specific reflective functioning; B = understandardized beta; β = standardized beta; SE = Standard error for the understandardized beta; P = probability value; CI = confidence intervals.
Discussion
Overall, the results confirm that the Trauma-specific reflective functioning scale applied to the Trauma Meaning-Making Interview is a valid and reliable instrument: it has strong psychometric properties, can be coded reliably, shows construct validity with an independent coding system of trauma-processing, is distinct and complementary to other related measures assessing reflective functioning or responses to trauma, and has a strong predictive validity using an observational measure of parental insightfulness.
Interestingly, T-RF was moderately associated with the accumulation of sociodemographic risk factors and with maternal education but was not associated with the type, timing and persistence of trauma. This is in line with previous studies observing no or weak associations between the severity of childhood maltreatment and RF or PRF in community samples (Garon-Bissonnette et al., Reference Garon-Bissonnette, Dubois-Comtois, St-Laurent and Berthelot2023; Huth-Bocks et al., Reference Huth-Bocks, Muzik, Beeghly, Earls and Stacks2014; Newman-Morris et al., Reference Newman-Morris, Simpson, Gray, Perry, Dunlop and Newman2020; Stacks et al., Reference Stacks, Muzik, Wong, Beeghly, Huth-Bocks, Irwin and Rosenblum2014; Taubner & Curth, Reference Taubner and Curth2013). This suggests that the complexity and severity of past traumas would not be the main determinant of adults’ capacities to think of these experiences and their repercussions in a coherent and meaningful way. In other words, our results suggest that some people who experienced isolated trauma still encounter significant difficulties in mentalizing this experience years later, whereas others, who experienced chronic cumulative traumas, show complex and articulate thinking processes regarding these experiences. This suggests that multiple intrapersonal (ex. intelligence, temperament, personality traits), interpersonal (ex. secure attachment relationships, positive peer relationships, social support) and community-level (supportive school environment, community social capita, availability of professional support) protective factors may provide the opportunity to keep on learning about oneself and others and to develop a coherent representation of one’s own traumatic experience (Afifi & MacMillan, Reference Afifi and MacMillan2011; Fonagy et al., Reference Fonagy, Campbell and Luyten2023; Racine et al., Reference Racine, Eirich and Madigan2022).
The findings provide novel insights concerning the protective role of mentalizing trauma. First, results showed a sturdy association between the complexity of thought processes in relation with past traumatic experiences and the mothers’ understanding of the psychological experience of their child during interactions. The association between T-RF and maternal insightfulness was observed for both positive and hostile maternal comments. Interestingly, neither maternal RF nor trauma-processing strategies, two other narrative measures, explained a unique part of the variance in maternal insightfulness. This supports the potentially unique contribution of T-RF to parenting and makes it unlikely that the observed associations are the mere result of shared method variance. Overall, these findings echoes Lieberman et al.’s (Reference Lieberman, Diaz, Castro and Bucio2020) and Narayan et al. (Reference Narayan, Bucio, Rivera and Lieberman2016) eloquent proposal that “making sense of the past creates space for the baby” in women who have experienced childhood trauma.
We also found that the two types of RF assessed in the current study (trauma-specific RF and parental RF) were moderately related and showed similar associations with other variables (see Table 2). However, only trauma-specific mentalization was significantly associated with positive comments and maternal hostility at the insightfulness assessment when entering both measures simultaneously in the model. This is in line with previous findings showing that mentalizing trauma explains a significant part of the variance in maternal engagement (Ensink et al., Reference Ensink, Berthelot, Bernazzani, Normandin and Fonagy2014) and the quality of the mother-infant attachment relationship (Berthelot et al., Reference Berthelot, Ensink, Bernazzani, Normandin, Luyten and Fonagy2015) that is not explained by attachment-based reflective functioning. Our results also offer additional empirical support to the proposal that making sense of trauma is particularly important to buffer against affective and behavioral dysregulation when the interaction with the child evokes overwhelming feelings in the parent (Dollberg & Hanetz-Gamliel, Reference Dollberg and Hanetz-Gamliel2023; Fonagy et al., Reference Fonagy, Campbell and Luyten2023). Under such circumstances where unmentalized mental states are reactivated (ex. shame, rage, helplessness), the parent may attempt to regulate internal feelings in a way that (a) will compete with the resources needed to respond adequately and with immediacy to the needs of the child, (b) involves the activation of a set of defensive strategies (ex. projective identification, dissociation, withdrawal) that impede or distort the parents’ appreciation of the child’s experience, and (c) may ultimately lead to hostile reactions against the source of the threat, the child, in an attempt to make it stop (Lieberman et al., Reference Lieberman, Diaz, Castro and Bucio2020; Schechter, Reference Schechter2019; Suardi et al., Reference Suardi, Rothenberg, Serpa and Schechter2017). In contrast, parents with good T-RF may be able to contain these threatening mental states and to properly attribute their source and intensity to their traumatic past rather than to their child’s behavior.
Second, we observed that our coding of T-RF yields significant associations with an independent coding system of trauma-processing strategies. Indeed, good T-RF positively correlated with constructive trauma-processing strategies and negatively correlated with avoidant strategies. However, T-RF was not associated with unresolved trauma-processing. This offers additional support to the previous observations that the two systems (U/d and T-RF) capture complementary mechanisms of healing from trauma (Ensink et al., Reference Ensink, Berthelot, Bernazzani, Normandin and Fonagy2014). Indeed, whereas the coding of unresolved trauma captures indices of disorientation or disorganization of reasoning, discourse and behavior, T-RF rather assesses the complexity of thought processes in relation to trauma. Accordingly, we have observed instances where the activation of trauma-related memory has led to lapses in the monitoring of discourse (ex. unusual attention to details, prolonged silences, unfinished sentences) or reports of extreme responses at the time of trauma, some of the indices captured by the unresolved/disorganized coding system, without significantly impacting one’s appreciation of mental states in relation to trauma. Conversely, more than half of the participants with organized, (i.e., not unresolved) trauma-processing strategies (n = 30; 54.5%) had poor or limited T-RF (scores < 5).
Third, contrary to our hypothesis, T-RF was not associated with the severity of depressive and post-traumatic symptoms. Despite strong conceptual links between deficits in RF and internalized disorders (Luyten et al., Reference Luyten, Lemma and Target2019), most studies that assessed mentalization using the reflective functioning scale similarly failed to document associations with PTSD or depression (Fischer-Kern et al., Reference Fischer-Kern, Kapusta, Doering, Hörz, Mikutta and Aigner2011; Schechter et al., Reference Schechter, Coots, Zeanah, Davies, Coates, Trabka, Marshall, Liebowitz and Myers2005; Suardi et al., Reference Suardi, Moser, Sancho Rossignol, Manini, Vital, Merminod, Kreis, Ansermet, Rusconi Serpa and Schechter2020) and some even documented a positive association (Suchman et al., Reference Suchman, DeCoste, Leigh and Borelli2010). The vast majority of findings showing that poor mentalization was associated with more severe depressive or post-traumatic symptoms indeed seem to be coming from studies using self-report measures of specific impairments in reflective functions (Berthelot et al., 2019, 2022; Fonagy et al., Reference Fonagy, Luyten, Moulton-Perkins, Lee, Warren, Howard, Ghinai, Fearon, Lowyck and Laws2016; Huang et al., Reference Huang, Fonagy, Feigenbaum, Montague and Nolte2020). This raises four possibilities. First, it may be that the distinctive failures in reflective processes (i.e., impaired and distorted mentalizing) that are assessed using self-report measures of mentalization such as the FMTQ (Berthelot et al., Reference Berthelot, Savard, Lemieux, Garon-Bissonnette, Ensink and Godbout2022) or the RFQ (Fonagy et al., Reference Fonagy, Luyten, Moulton-Perkins, Lee, Warren, Howard, Ghinai, Fearon, Lowyck and Laws2016), may be more useful for our understanding of psychopathology than interview-based assessments of RF which assess the complexity of reflective processes. Second, self-report measures of RF may be more strongly influenced by neuroticism and negative cognitive biases than narrative measures. Third, it may be that mentalizing is associated with an increased sensitivity to difficult emotions and a lowered used of defense mechanisms aiming to keep at distance uncomfortable thoughts and feelings (Slade & Steele, Reference Slade and Sleed2024). Consequently, some participants with preserved mentalization abilities may be likely to endorse some level of depressed and anxious moods and cognition at self-reported instruments. This hypothesis is in line with Simon et al.’s (Reference Simon, Feiring and Kobielski McElroy2010) observation that the youth who have coherent representations of their traumatic experiences are not protected from experiencing ongoing distress as they process abuse-related mental states. However, they differ from the youth with more problematic trauma-processing strategies in that they remain open to exploring their experience and attempt different coping strategies to regulate overwhelming feelings. Finally, our recent findings using the Failure to Mentalize Trauma Questionnaire (Berthelot & Garon-Bissonnette, Reference Berthelot and Garon-Bissonnette2024) highlighted important heterogeneity in terms of the specific failures in mentalizing trauma expressed by participants at the lower end of the T-RF scale and showed that specific types of failures in mentalizing trauma predicted specific sets of symptoms and dysfunctions. Therefore, it may be that only some types of disruptions in mentalizing trauma are associated with internalized symptoms and that our ability to detect these associations in the current study was limited by the exclusive reliance on a global score of T-RF.
Taken together, our findings and those of previous studies (Ensink et al., Reference Ensink, Berthelot, Bernazzani, Normandin and Fonagy2014; Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2003) suggest that the resolution of trauma is a highly complex multifaceted construct involving distinct and independent abilities and components, each capturing a unique part of the larger picture and probably having specific determinants and correlates. This is highlighted in the current study where we showed that absorbed and avoidant trauma-processing strategies were associated with psychopathology but not maternal insightfulness, whereas T-RF was not associated with self-reported symptoms of depression and PTSD but emerged as a very strong correlate of parenting (here measured through maternal insightfulness). Interestingly, other operationalizations of the resolution of trauma, such as Swerbenski’s novel coding scheme applied to the PDI, found that higher acceptance and forgiveness held by mothers toward their primary caregiver was associated with lower depressive symptoms and higher maternal sensitivity. This calls for future studies investigating the contribution of T-RF to parenting and healing from trauma alongside other relevant operationalization of (un)resolved trauma, such as acceptance and forgiveness (Swerbenski et al., Reference Swerbenski, Sturge-Apple, Messina, Toth, Rogosch and Cicchetti2023), hostile-helpless representations (Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2005), unresolved/disorganized states of mind, and psychophysiological stress responses (Bakkum et al., Reference Bakkum, Oosterman, Verhage, Kunseler, Fearon, Schuengel and Duschinsky2022).
Limitations
The study has several strengths including the use of gold standard observational measures of trauma-processing strategies, parental reflective functioning, trauma-specific reflective functioning and maternal insightfulness, all coded blind to other measures by independent coders. The findings of this study need to be interpreted in the light of some limitations. First, the study largely relied on narrative measures and we cannot rule out that associations between variables could be partly explained by participants’ verbal abilities which were not assessed using an independent measure. However, we considered two proxies for verbal abilities (number of words during the TMMIs and maternal education) which revealed that the length of transcripts was not associated with reflective functioning and that T-RF was associated with PRF and maternal insightfulness over and beyond the effect of education status. Second, although PRF was shown to be fairly stable over time (Malcorps et al., Reference Malcorps, Vliegen, Fonagy and Luyten2022), the fact that PRF was not evaluated concurrently with other variables may have affected the strength of the correlations. The finding that T-RF would be a better proxy for maternal understanding of her child in an affectively hot context, as measured using the insightfulness assessment, than PRF will thus have to be confirmed by future studies using cross-sectional assessments of the three concepts. Third, the findings of the study may not be generalizable to all caregivers, such as fathers, or to women who have experienced other types of trauma than childhood abuse and neglect (e.g., migration trajectories, domestic violence). Fourth, although the sample was rather large in comparison to other studies of trauma-exposed mother-infant dyads using observational measures (Berthelot et al., Reference Berthelot, Ensink, Bernazzani, Normandin, Luyten and Fonagy2015; Ensink et al., Reference Ensink, Normandin, Target, Fonagy, Sabourin and Berthelot2015; Frigerio et al., Reference Frigerio, Costantino, Ceppi and Barone2013; Lyons-Ruth et al., Reference Lyons-Ruth, Yellin, Melnick and Atwood2005), a larger sample would have eliminated possible type 2 errors. Fifth, T-RF may protect against externalized symptoms more so than protecting against internalized problems. However, this could not be tested in the current study since only PTSD and depression were assessed. Sixth, further studies should examine the contribution of T-RF, PRF and trauma-processing strategies to maternal behaviors, mother-infant attachment and child development. Seventh, some limitations inherent to retrospective measures, such as recall biases, may apply to the current study and affect T-RF scores, notably during the first section of the TMMI which specifically addresses the experience of trauma. Finally, in light of recent findings linking distinctive failures in the mentalization of trauma assessed using the FMTQ to specific internalized and externalized symptoms (Berthelot & Garon-Bissonnette, Reference Berthelot and Garon-Bissonnette2024), using the FMTQ in addition to the T-RF coding system could have helped clarify the complex association between poor reflective functioning and psychopathology.
Clinical implications
Taken together, our findings suggest that having a good understanding of trauma and its impact would exert a strong positive effect in relationship with others, namely the child, but may have a limited protective effect for the self. If such findings are eventually confirmed by other studies, this could contribute to the emergence of a new model of personalized medicine for survivors of trauma. For instance, a person manifesting disturbances in relationships with others as a result of trauma may particularly benefit from psychotherapies targeting the mentalization of trauma, whereas another person who has preserved relationships but struggles with internalized symptoms may benefit from other types of interventions aiming to calm physiological reactivity.
The current study also offers some support to Suchman et al.’s (Reference Suchman, DeCoste, Leigh and Borelli2010) three-step processes for intervention with vulnerable parents. This model suggests that clinical practices should primarily focus on impairments in self-mentalization in the parents, before targeting interpersonal (or child-focused) mentalization and providing information and guidance. Indeed, our observation that T-RF was especially predictive of maternal insightfulness and maternal hostility and was prospectively associated with maternal reflective functioning in mothers who had experienced child abuse or neglect suggests that making sense of trauma may be an important first step to increasing emotional availability in mothers and to help them contain trauma-related mental states when such feelings and cognitions are activated in the mother-infant relationship. Our findings also support the idea that parents who experienced childhood trauma may particularly benefit from specific parenting interventions addressing trauma and its impact. Ideally, such interventions should be offered before childbirth to prevent the imbrication of trauma in the mother-infant relationship. Future research should evaluate whether prenatal programs such as the Perinatal Child-Parent Psychotherapy (Lieberman et al., Reference Lieberman, Diaz, Castro and Bucio2020), STEP (Supporting the Transition to and Engagement in Parenthood; Berthelot et al., Reference Berthelot, Drouin-Maziade, Garon-Bissonnette, Lemieux, Sériès and Lacharité2021; Reference Berthelot, Larouche, Garon-Bissonnette, Deschênes, Drouin-Maziade and Lemieux2024) or The Survivor Moms’ Companion (Sperlich & Kabilamany, Reference Sperlich and Kabilamany2022), or postnatal interventions such as Mom Power (Rosenblum et al., Reference Rosenblum, Lawler, Alfafara, Miller, Schuster and Muzik2017, Reference Rosenblum, Muzik, Morelen, Alfafara, Miller, Waddell, Schuster and Ribaudo2018) or Attachment and Child Health (ATTACH, Letourneau et al., Reference Letourneau, Anis, Ntanda, Novick, Steele, Steele and Hart2020) contribute to mitigate the intergenerational repercussions of childhood trauma through an enrichment of trauma-specific mentalization.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S095457942400110X
Acknowledgements
This work was supported by the Social Sciences and Humanities Research Council of Canada (grant #430-2017-00994, Principal Investigator, N.B.), the Canada Research Chair in Developmental Trauma (grant #950-232739, Principal Investigator, N.B.), the National Institute of Mental Health and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant #MH080147; Principal Investigator, M.M.) and the Michigan Institute for Clinical and Health Research at the University of Michigan (grant #UL1RR024986; Principal Investigator, M.M.). We thank the mothers and children who made this research possible and gratefully acknowledge the contributions of Amanda Fezzey, Heather Cameron, Alexi Wisher, Lauren Earls, Lori Stark, Ryan Hill, Kayla Frick, and Alex Busuito.
Competing interests
The authors have no conflict of interest to declare.








 Open access
Open access